

A case of mid-apical obstructive hypertrophic cardiomyopathy treated with a transapical myectomy approach: a case report
- PMID: 25384531
- PMCID: PMC4232228
- DOI: 10.1186/1752-1947-8-364
A case of mid-apical obstructive hypertrophic cardiomyopathy treated with a transapical myectomy approach: a case report
Abstract
Introduction: Hypertrophic cardiomyopathy is a genetic cardiac disease characterized by marked variability in morphological expression and natural history. The hypertrophic myocardium is often confined to the septum or lateral wall of the left ventricle, but it can also be encountered in the middle or apical segments of the myocardium. Treatment is based on medical therapy. Others therapies, such as embolization of the septal artery or ventriculomyectomy, are indicated in special situations. Surgery is the standard treatment, and it is classically done via a transaortic approach; however, in cases in which the hypertrophic myocardium is confined to mid-apical segments, a transapical approach is an option. Only a few cases of mid-apical obstructive hypertrophic cardiomyopathy treated with a myectomy using a transapical approach have been reported in the English-language literature. In this report, we present a case of a patient with mid-apical obstructive hypertrophic cardiomyopathy treated using this new approach.
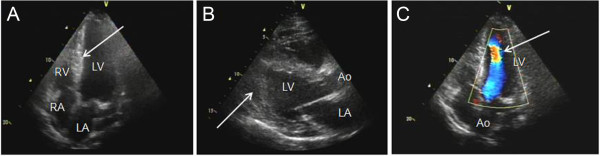
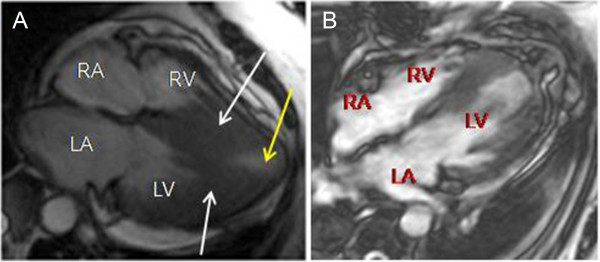
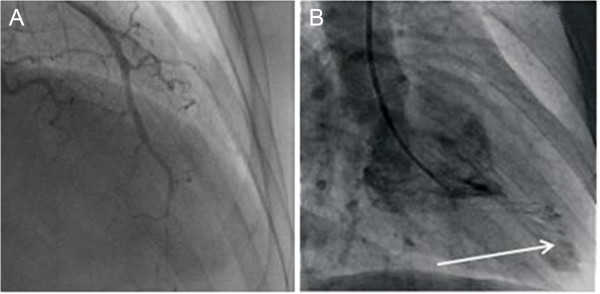
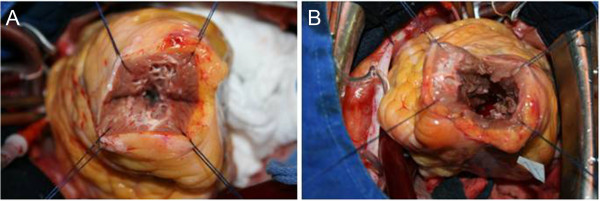
Case presentation: A 63-year-old Caucasian woman presented with a history of chest pain and shortness of breath causing significant limitations on her daily life activities. She had a history of coronary artery disease. Her physical examination was unremarkable. Transthoracic echocardiography revealed normal systolic function and significant concentric left ventricular hypertrophy that was greater in the mid-apical region. Nuclear magnetic resonance imaging confirmed significant hypertrophy of the median segments of the left ventricle. The patient had persistent symptoms despite receiving optimized medical treatment, and a surgical approach was indicated. As a myectomy using transaortic technique was thought to be difficult to perform in her case, a transapical approach was used. No complications occurred, and her symptoms resolved.
Conclusion: A transapical myectomy should be taken into consideration for patients with mid-apical obstructive hypertrophic cardiomyopathy that is refractory to medical treatment.
Figures
References
-
- Maron BJ. Hypertrophic cardiomyopathy: a systematic review. JAMA. 2002;287:1308–1320. - PubMed
-
- Efthimiadis GK, Pagourelias ED, Parcharidou D, Gossios T, Kamperidis V, Theofilogiannakos EK, Pappa Z, Meditskou S, Hadjimiltiades S, Pliakos C, Karvounis H, Styliadis IH. Clinical characteristics and natural history of hypertrophic cardiomyopathy with midventricular obstruction. Circ J. 2013;77:2366–2374. doi: 10.1253/circj.CJ-12-1561. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
