

Use of a pathway quality improvement care bundle to reduce mortality after emergency laparotomy
- PMID: 25384994
- PMCID: PMC4312892
- DOI: 10.1002/bjs.9658
Use of a pathway quality improvement care bundle to reduce mortality after emergency laparotomy
Abstract
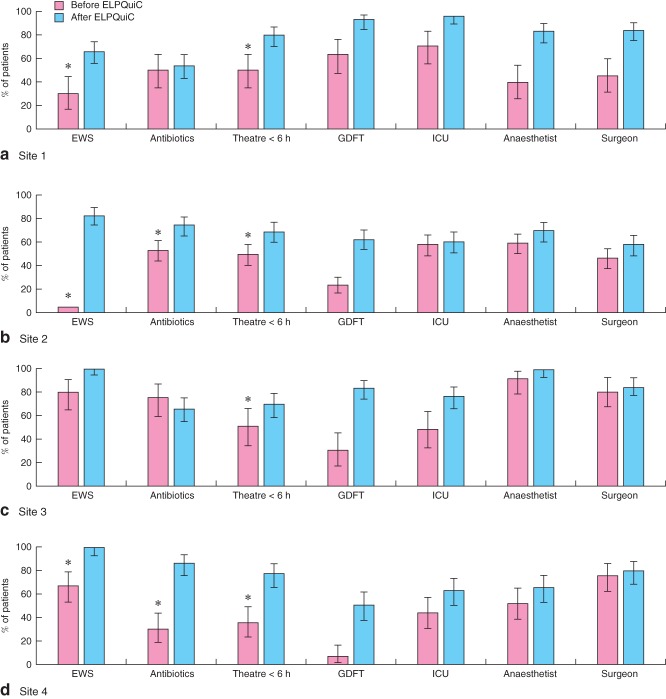
Background: Emergency laparotomies in the U.K., U.S.A. and Denmark are known to have a high risk of death, with accompanying evidence of suboptimal care. The emergency laparotomy pathway quality improvement care (ELPQuiC) bundle is an evidence-based care bundle for patients undergoing emergency laparotomy, consisting of: initial assessment with early warning scores, early antibiotics, interval between decision and operation less than 6 h, goal-directed fluid therapy and postoperative intensive care.
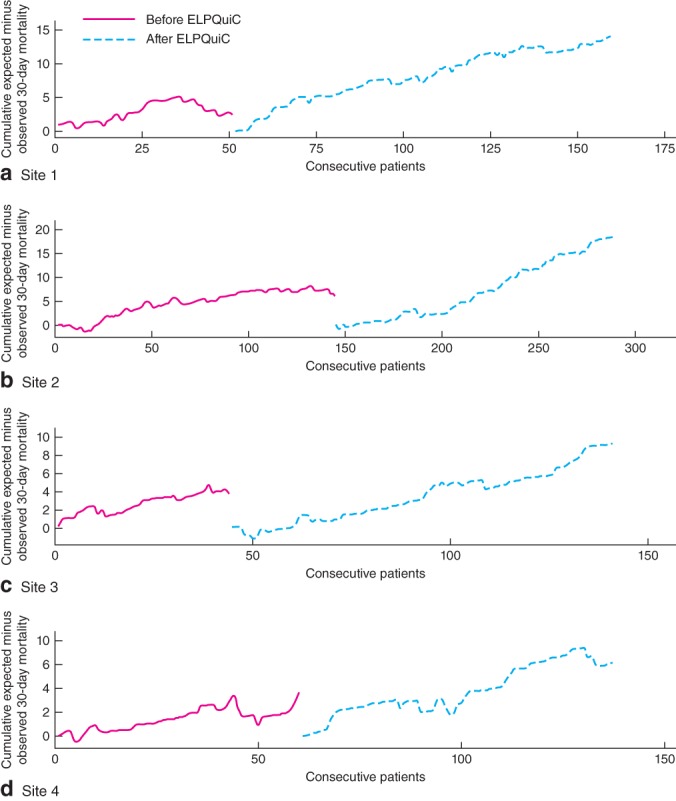
Methods: The ELPQuiC bundle was implemented in four hospitals, using locally identified strategies to assess the impact on risk-adjusted mortality. Comparison of case mix-adjusted 30-day mortality rates before and after care-bundle implementation was made using risk-adjusted cumulative sum (CUSUM) plots and a logistic regression model.
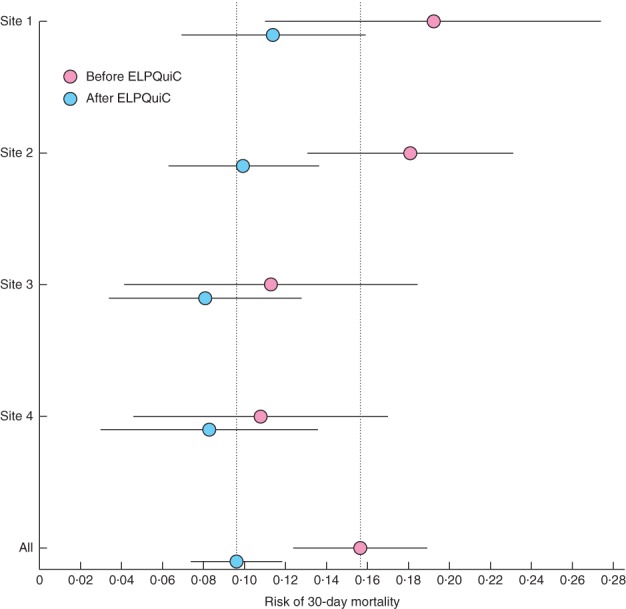
Results: Risk-adjusted CUSUM plots showed an increase in the numbers of lives saved per 100 patients treated in all hospitals, from 6.47 in the baseline interval (299 patients included) to 12.44 after implementation (427 patients included) (P < 0.001). The overall case mix-adjusted risk of death decreased from 15.6 to 9.6 per cent (risk ratio 0.614, 95 per cent c.i. 0.451 to 0.836; P = 0.002). There was an increase in the uptake of the ELPQuiC processes but no significant difference in the patient case-mix profile as determined by the mean Portsmouth Physiological and Operative Severity Score for the enUmeration of Mortality and morbidity risk (0.197 and 0.223 before and after implementation respectively; P = 0.395).
Conclusion: Use of the ELPQuiC bundle was associated with a significant reduction in the risk of death following emergency laparotomy.
© 2014 The Authors. BJS published by John Wiley & Sons Ltd on behalf of BJS Society Ltd.
Figures
References
-
- Shafi S, Aboutanos MB, Agarwal S, Brown CVR, Crandall M, Feliciano DV, et al. AAST Committee on Severity Assessment and Patient Outcomes. Emergency general surgery: definition and estimated burden of disease. J Trauma Acute Care Surg. 2013;74:1092–1097. - PubMed
-
- Shapter SL, Paul MJ, White SM. Incidence and annual cost of emergency laparotomy in England: is there a major funding shortfall? Anaesthesia. 2012;67:474–478. - PubMed
-
- Saunders DI, Murray D, Pichel AC, Varley S, Peden CJ. Variations in mortality after emergency laparotomy: the first report of the UK Emergency Laparotomy Network. Br J Anaesth. 2012;109:368–375. - PubMed
-
- Al-Temimi MH, Griffee M, Enniss TM, Preston R, Vargo D, Overton S, et al. When is death inevitable after emergency laparotomy? Analysis of the American College of Surgeons National Surgical Quality Improvement Program database. J Am Coll Surg. 2012;215:503–511. - PubMed
-
- Vester-Andersen M, Lundstrøm LH, Møller MH, Waldau T, Rosenberg J, Møller AM, Danish Anaesthesia Database Mortality and postoperative care pathways after emergency gastrointestinal surgery in 2904 patients: a population-based cohort study. Br J Anaesth. 2014;112:860–870. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
