

Signatures of tumour immunity distinguish Asian and non-Asian gastric adenocarcinomas
- PMID: 25385008
- PMCID: PMC4680172
- DOI: 10.1136/gutjnl-2014-308252
Signatures of tumour immunity distinguish Asian and non-Asian gastric adenocarcinomas
Abstract
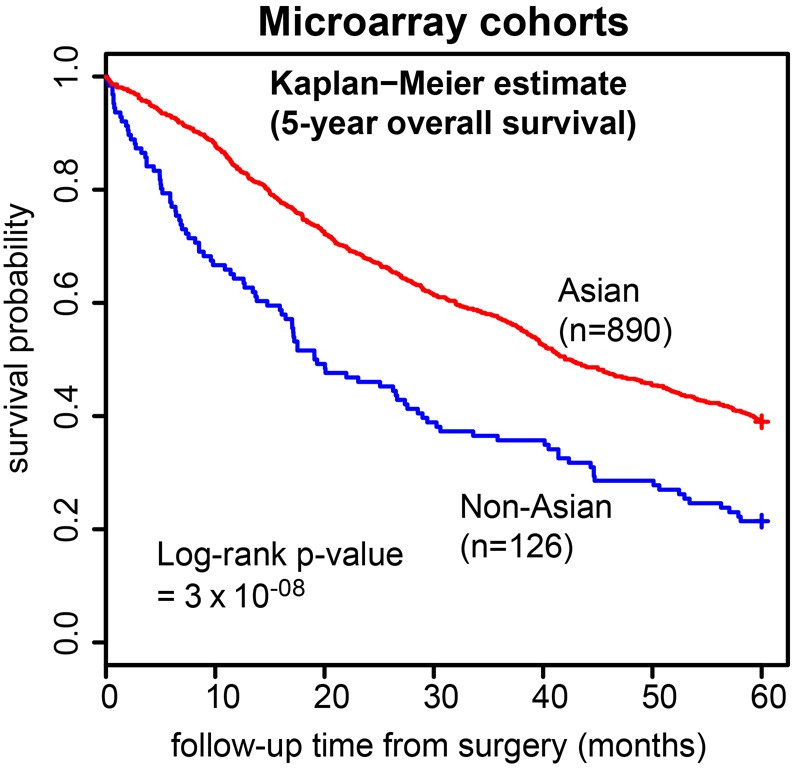
Objective: Differences in gastric cancer (GC) clinical outcomes between patients in Asian and non-Asian countries has been historically attributed to variability in clinical management. However, recent international Phase III trials suggest that even with standardised treatments, GC outcomes differ by geography. Here, we investigated gene expression differences between Asian and non-Asian GCs, and if these molecular differences might influence clinical outcome.
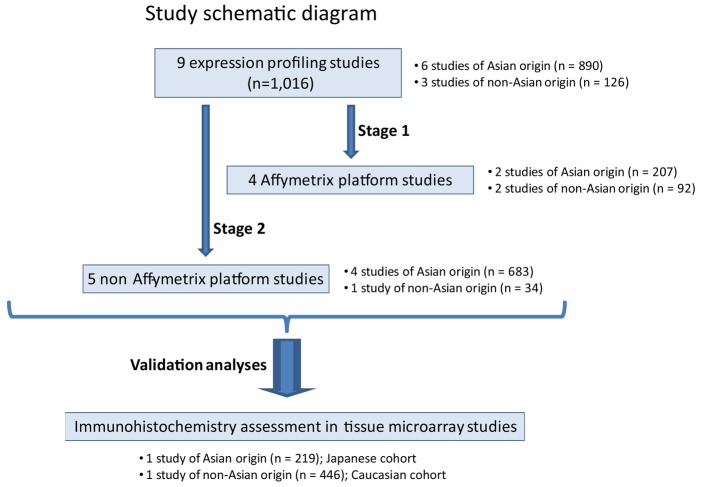
Design: We compared gene expression profiles of 1016 GCs from six Asian and three non-Asian GC cohorts, using a two-stage meta-analysis design and a novel biostatistical method (RUV-4) to adjust for technical variation between cohorts. We further validated our findings by computerised immunohistochemical analysis on two independent tissue microarray (TMA) cohorts from Asian and non-Asian localities (n=665).
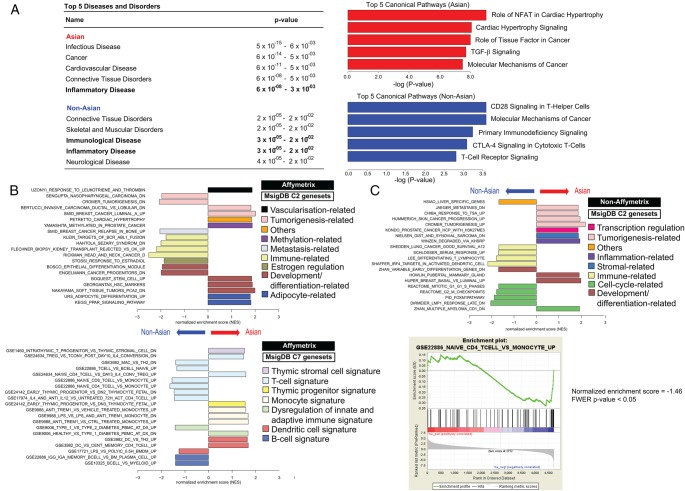
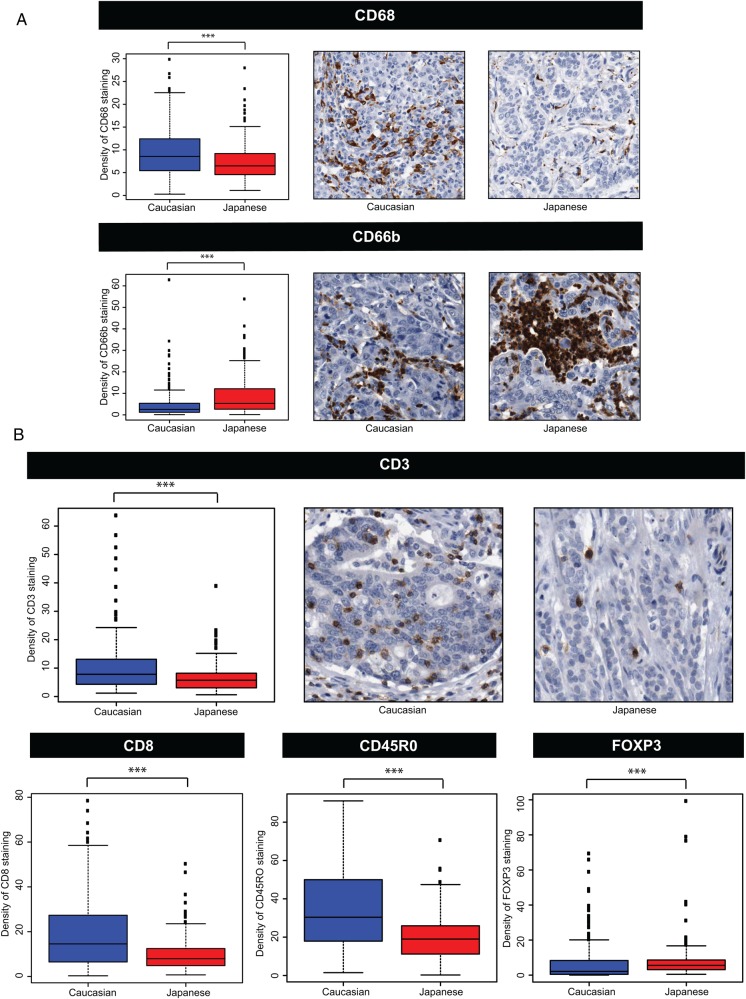
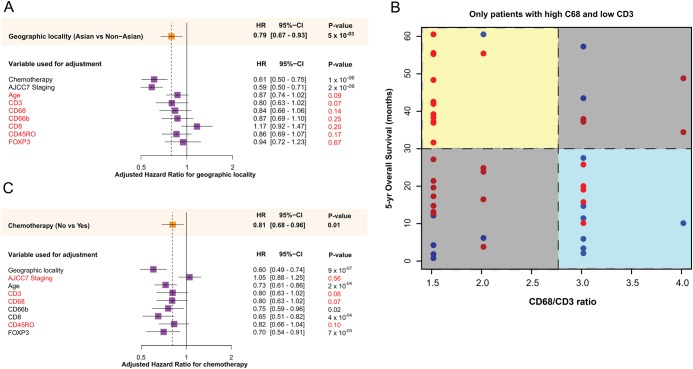
Results: Gene signatures differentially expressed between Asians and non-Asian GCs were related to immune function and inflammation. Non-Asian GCs were significantly enriched in signatures related to T-cell biology, including CTLA-4 signalling. Similarly, in the TMA cohorts, non-Asian GCs showed significantly higher expression of T-cell markers (CD3, CD45R0, CD8) and lower expression of the immunosuppressive T-regulatory cell marker FOXP3 compared to Asian GCs (p<0.05). Inflammatory cell markers CD66b and CD68 also exhibited significant cohort differences (p<0.05). Exploratory analyses revealed a significant relationship between tumour immunity factors, geographic locality-specific prognosis, and postchemotherapy outcomes.
Conclusions: Analyses of >1600 GCs suggest that Asian and non-Asian GCs exhibit distinct tumour immunity signatures related to T-cell function. These differences may influence geographical differences in clinical outcome, and the design of future trials particularly in immuno-oncology.
Keywords: GASTRIC CANCER; GENE EXPRESSION; IMMUNOLOGY; MOLECULAR MECHANISMS; MOLECULAR PATHOLOGY.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Figures
Comment in
-
Ethnicity-related differences in tumor immunity: a new possible explanation for gastric cancer prognostic variability?Transl Gastroenterol Hepatol. 2016 Mar 16;1:11. doi: 10.21037/tgh.2016.03.03. eCollection 2016. Transl Gastroenterol Hepatol. 2016. PMID: 28138578 Free PMC article. No abstract available.
References
-
- Ferlay J, Soerjomataram I, Ervik M, et al. . Cancer Incidence and Mortality Worldwide: IARC CancerBase No. 11 2013.
-
- Greenlee RT, Hill-Harmon MB, Murray T, et al. . Cancer statistics, 2001. CA Cancer J Clin 2001;51:15–36. - PubMed
-
- Lee WJ, Lee WC, Houng SJ, et al. . Survival after resection of gastric cancer and prognostic relevance of systematic lymph node dissection: twenty years experience in Taiwan. World J Surg 1995;19:707–13. - PubMed
-
- Mok YJ, Koo BW, Whang CW, et al. . Cancer of the stomach: a review of two hospitals in Korea and Japan. World J Surg 1993;17:777–82. - PubMed
-
- Fuchs CS, Mayer RJ. Gastric carcinoma. N Engl J Med 1995;333:32–41. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous