

Approaches to ventilation in intensive care
- PMID: 25385483
- PMCID: PMC4233762
- DOI: 10.3238/arztebl.2014.0714
Approaches to ventilation in intensive care
Abstract
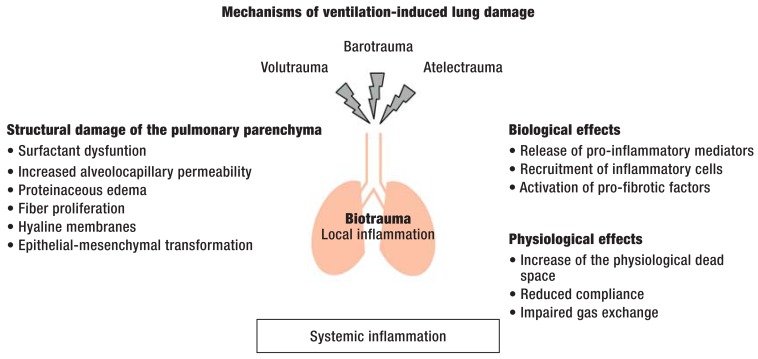
Background: Mechanical ventilation is a common and often life-saving intervention in intensive care medicine. About 35% of all patients in intensive care are mechanically ventilated; about 15% of these patients develop a ventilation-associated pneumonia. The goal of ventilation therapy is to lessen the work of respiration and pulmonary gas exchange and thereby maintain or restore an adequate oxygen supply to the body's tissues. Mechanical ventilation can be carried out in many different modes; the avoidance of ventilation-induced lung damage through protective ventilation strategies is currently a major focus of clinical interest.
Method: This review is based on pertinent articles retrieved by a selective literature search.
Results: Compared to conventional lung-protecting modes of mechanical ventilation, the modern modes of ventilation presented here are further developments that optimize lung protection while improving pulmonary function and the synchrony of the patient with the ventilator. In high-frequency ventilation, tidal volumes of 1-2 mL/kgBW (body weight) are given, at a respiratory rate of up to 12 Hz. Assisted forms of spontaneous respiration are also in use, such as proportional assist ventilation (PAV), neurally adjusted ventilatory assist (NAVA), and variable pressure-support ventilation. Computer-guided closed-loop ventilation systems enable automated ventilation; according to a recent meta-analysis, they shorten weaning times by 32% .
Conclusion: The currently available scientific evidence with respect to clinically relevant endpoints is inadequate for all of these newer modes of ventilation. It appears, however, that they can lower both the invasiveness and the duration of mechanical ventilation, and thus improve the care of patients who need ventilation. Randomized trials with clinically relevant endpoints must be carried out before any final judgments can be made.
Figures
Similar articles
-
Neurally adjusted ventilatory assist: a ventilation tool or a ventilation toy?Respir Care. 2011 Mar;56(3):327-35. doi: 10.4187/respcare.00775. Epub 2011 Jan 21. Respir Care. 2011. PMID: 21255496 Review.
-
Mechanical ventilation of the premature neonate.Respir Care. 2011 Sep;56(9):1298-311; discussion 1311-3. doi: 10.4187/respcare.01429. Respir Care. 2011. PMID: 21944682 Review.
-
Nontraditional modes of mechanical ventilation: progress or distraction?Expert Rev Respir Med. 2012 Jun;6(3):277-84. doi: 10.1586/ers.12.25. Expert Rev Respir Med. 2012. PMID: 22788942 Review.
-
Advanced closed loops during mechanical ventilation (PAV, NAVA, ASV, SmartCare).Best Pract Res Clin Anaesthesiol. 2009 Mar;23(1):81-93. doi: 10.1016/j.bpa.2008.08.001. Best Pract Res Clin Anaesthesiol. 2009. PMID: 19449618 Review.
-
Proportional assist ventilation and neurally adjusted ventilatory assist.Respir Care. 2011 Feb;56(2):140-8; discussion 149-52. doi: 10.4187/respcare.01021. Respir Care. 2011. PMID: 21333175 Review.
Cited by
-
Management of Chronic Obstructive Pulmonary Disease (COPD) Exacerbations in Hospitalized Patients From Admission to Discharge: A Comprehensive Review of Therapeutic Interventions.Cureus. 2023 Aug 18;15(8):e43694. doi: 10.7759/cureus.43694. eCollection 2023 Aug. Cureus. 2023. PMID: 37724212 Free PMC article. Review.
-
Sequential invasive-noninvasive mechanical ventilation weaning strategy for patients after tracheostomy.World J Emerg Med. 2015;6(3):196-200. doi: 10.5847/wjem.j.1920-8642.2015.03.006. World J Emerg Med. 2015. PMID: 26401180 Free PMC article.
-
Clinical characteristics and outcomes of cancer patients requiring intensive care unit admission: a prospective study.J Cancer Res Clin Oncol. 2018 Apr;144(4):717-723. doi: 10.1007/s00432-018-2581-0. Epub 2018 Jan 23. J Cancer Res Clin Oncol. 2018. PMID: 29362918 Free PMC article.
-
Severe thoracic trauma - still an independent predictor for death in multiple injured patients?Scand J Trauma Resusc Emerg Med. 2018 Jan 8;26(1):6. doi: 10.1186/s13049-017-0469-7. Scand J Trauma Resusc Emerg Med. 2018. PMID: 29310701 Free PMC article.
-
[Acute respiratory distress syndrome : Basic principles and treatment].Anaesthesist. 2017 Jul;66(7):539-552. doi: 10.1007/s00101-017-0337-x. Anaesthesist. 2017. PMID: 28677019 Review. German.
References
-
- Esteban A, Frutos-Vivar F, Muriel A, et al. Evolution of mortality over time in patients receiving mechanical ventilation. Am J Respir Crit Care Med. 2013;188:220–230. - PubMed
-
- Wunsch H, Linde-Zwirble WT, Angus DC, Hartman ME, Milbrandt EB, Kahn JM. The epidemiology of mechanical ventilation use in the United States. Crit Care Med. 2010;38:1947–1953. - PubMed
-
- Slutsky AS, Ranieri VM. Ventilator-induced lung injury. N Engl J Med. 2013;369:2126–2136. - PubMed
-
- Craven DE, Lei Y, Ruthazer R, Sarwar A, Hudcova J. Incidence and outcomes of ventilator-associated tracheobronchitis and pneumonia. AJM. 2013;126:542–549. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical