

Malignant gangliocytic paraganglioma of the duodenum with distant metastases and a lethal course
- PMID: 25386095
- PMCID: PMC4223280
- DOI: 10.3748/wjg.v20.i41.15454
Malignant gangliocytic paraganglioma of the duodenum with distant metastases and a lethal course
Abstract
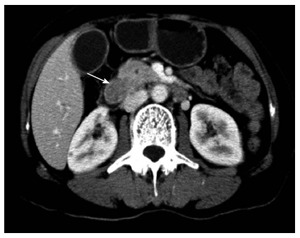
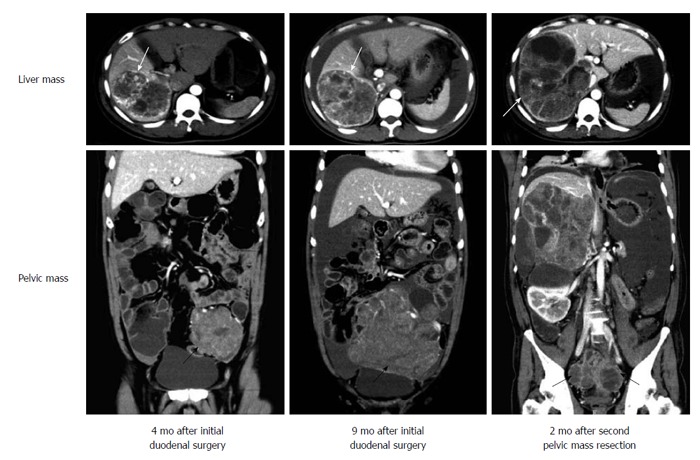
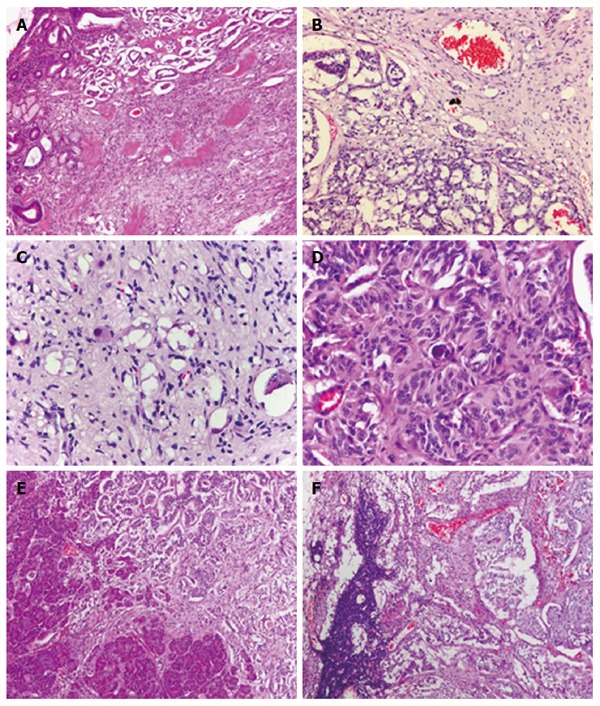
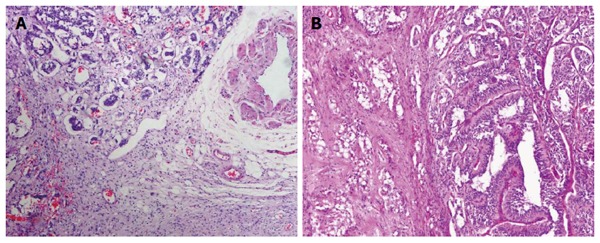
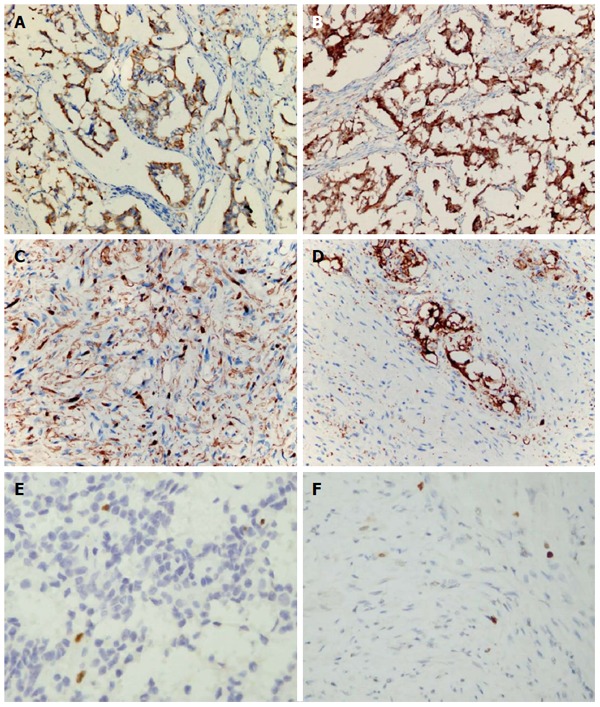
Gangliocytic paraganglioma (GP) is rare and has been regarded as benign in general with a good prognosis. We present a patient with duodenal GP showing a malignant and lethal clinical course. A 47-year-old male patient was found to have a duodenal tumor and enlarged regional lymph nodes. The patient initially underwent a pancreaticoduodenectomy to resect the tumor and involved lymph nodes completely. Histological and immunohistochemical analyses showed findings typical of GP. However, the distant metastatic lesions in the liver and pelvic cavity were rapidly observed after surgery. The patient underwent chemotherapy and radiotherapy, as well as a second surgery to partly remove the metastatic mass in the pelvic cavity. The histological examination revealed no significant difference in histological features between the primary duodenal tumor and the metastatic pelvic mass. However, the patient finally died of the tumor due to the recurrence of the residual pelvic lesion and increased liver mass. To our knowledge, this is the first report of lethal GP with multifocal metastases. Our case confirms that GP should be regarded as a malignant potential tumor with behavior code of "1", rather than a benign tumor of "0".
Keywords: Duodenal neoplasms; Gangliocytic neoplasms; Lymphatic metastasis; Paraganglioma; Treatment outcome.
Figures
Similar articles
-
Gangliocytic paraganglioma: a rare case with metastases of all 3 elements to liver and lymph nodes.Ann Diagn Pathol. 2011 Dec;15(6):467-71. doi: 10.1016/j.anndiagpath.2010.07.009. Epub 2010 Oct 30. Ann Diagn Pathol. 2011. PMID: 21036639
-
Duodenal gangliocytic paraganglioma showing lymph node metastasis: a rare case report.Diagn Pathol. 2010 May 6;5:27. doi: 10.1186/1746-1596-5-27. Diagn Pathol. 2010. PMID: 20444291 Free PMC article.
-
Duodenal gangliocytic paraganglioma with lymph node metastasis and an 8-year follow-up: a case report.Eur J Gastroenterol Hepatol. 2012 Jan;24(1):90-4. doi: 10.1097/MEG.0b013e32834dfdfa. Eur J Gastroenterol Hepatol. 2012. PMID: 22081010
-
Duodenal gangliocytic paraganglioma: report of two cases and review of literature.Int J Clin Exp Pathol. 2015 Sep 1;8(9):9752-9. eCollection 2015. Int J Clin Exp Pathol. 2015. PMID: 26617685 Free PMC article. Review.
-
Gangliocytic paraganglioma: case report and review of the literature.J Gastrointest Surg. 2007 Oct;11(10):1351-4. doi: 10.1007/s11605-007-0217-9. Epub 2007 Jul 25. J Gastrointest Surg. 2007. PMID: 17653595 Review.
Cited by
-
Treatment and management of duodenal gangliocytic paraganglioma: A case report.Exp Ther Med. 2024 Sep 19;28(6):435. doi: 10.3892/etm.2024.12723. eCollection 2024 Dec. Exp Ther Med. 2024. PMID: 39355522 Free PMC article.
-
Gangliocytic paraganglioma: a multi-institutional retrospective study in Japan.BMC Cancer. 2015 Apr 12;15:269. doi: 10.1186/s12885-015-1308-8. BMC Cancer. 2015. PMID: 25886293 Free PMC article.
-
Duodenal gangliocytic paraganglioma, successfully treated by local surgical excision-a case report.Int J Surg Case Rep. 2017;32:5-8. doi: 10.1016/j.ijscr.2017.01.046. Epub 2017 Jan 19. Int J Surg Case Rep. 2017. PMID: 28213067 Free PMC article.
-
Diagnosis, Pathological Findings, and Clinical Management of Gangliocytic Paraganglioma: A Systematic Review.Front Oncol. 2018 Jul 27;8:291. doi: 10.3389/fonc.2018.00291. eCollection 2018. Front Oncol. 2018. PMID: 30101131 Free PMC article.
-
Gangliocytic paraganglioma: An overview and future perspective.World J Clin Oncol. 2019 Sep 24;10(9):300-302. doi: 10.5306/wjco.v10.i9.300. World J Clin Oncol. 2019. PMID: 31572665 Free PMC article.
References
-
- Kloppel G, Arnold R, Capella C, Klimstra DS, Albores-Saavedra J, Solcia E, Rindi G, Komminoth R. Neruoendocrine neoplasms of the ampullary region. In: Bosman FT, Carneiro F, Hruban RH, editors. WHO classification of the tumors of the digestive system. Lyon: IARC press; 2010. pp. 92–94.
-
- Büchler M, Malfertheiner P, Baczako K, Krautzberger W, Beger HG. A metastatic endocrine-neurogenic tumor of the ampulla of Vater with multiple endocrine immunoreaction--malignant paraganglioma? Digestion. 1985;31:54–59. - PubMed
-
- Korbi S, Kapanci Y, Widgren S. [Malignant paraganglioma of the duodenum. Immunohistochemical and ultrastructural study of a case] Ann Pathol. 1987;7:47–55. - PubMed
-
- Inai K, Kobuke T, Yonehara S, Tokuoka S. Duodenal gangliocytic paraganglioma with lymph node metastasis in a 17-year-old boy. Cancer. 1989;63:2540–2545. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
