

The initial response to the Boston marathon bombing: lessons learned to prepare for the next disaster
- PMID: 25386862
- PMCID: PMC5531449
- DOI: 10.1097/SLA.0000000000000914
The initial response to the Boston marathon bombing: lessons learned to prepare for the next disaster
Abstract
Objective: We discuss the strengths of the medical response to the Boston Marathon bombings that led to the excellent outcomes. Potential shortcomings were recognized, and lessons learned will provide a foundation for further improvements applicable to all institutions.
Background: Multiple casualty incidents from natural or man-made incidents remain a constant global threat. Adequate preparation and the appropriate alignment of resources with immediate needs remain the key to optimal outcomes.
Methods: A collaborative effort among Boston's trauma centers (2 level I adult, 3 combined level I adult/pediatric, 1 freestanding level I pediatric) examined the details and outcomes of the initial response. Each center entered its respective data into a central database (REDCap), and the data were analyzed to determine various prehospital and early in-hospital clinical and logistical parameters that collectively define the citywide medical response to the terrorist attack.
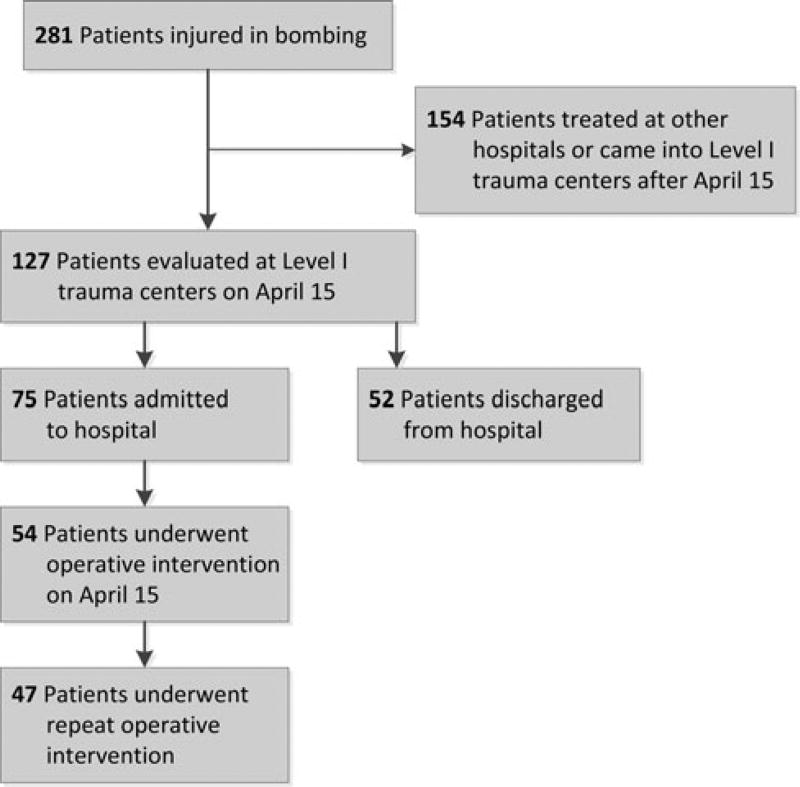
Results: A total of 281 people were injured, and 127 patients received care at the participating trauma centers on that day. There were 3 (1%) immediate fatalities at the scene and no in-hospital mortality. A majority of the patients admitted (66.6%) suffered lower extremity soft tissue and bony injuries, and 31 had evidence for exsanguinating hemorrhage, with field tourniquets in place in 26 patients. Of the 75 patients admitted, 54 underwent urgent surgical intervention and 12 (22%) underwent amputation of a lower extremity.
Conclusions: Adequate preparation, rapid logistical response, short transport times, immediate access to operating rooms, methodical multidisciplinary care delivery, and good fortune contributed to excellent outcomes.
Conflict of interest statement
Disclosure: The authors declare that there are no conflicts of interest and that no funding was received in support of this manuscript.
Figures
References
-
- Shariat S, Stennies G, Waxweiler R, et al. Physical injuries and fatalities resulting from the Oklahoma City bombing. JAMA. 1996;276:382–387. - PubMed
-
- Cushman JG, Pachter HL, Beaton HL, et al. Two New York City hospitals’ surgical response to the September 11, 2001, terrorist attack in New York City. J Trauma. 2003;54:147–154. discussion 154–155. - PubMed
-
- Feliciano DV, Anderson GV, Jr, Rozycki GS, et al. Management of casualties from the bombing at the centennial Olympics. Am J Surg. 1998;6:538–543. - PubMed
-
- U.S. Department of Commerce. United States Census Bureau. [Accessed August 31, 2013]; Available at: http://quickfacts.census.gov/qfd/states/25/2507000.html.
-
- Caterson EJ, Carty M, Weaver MJ, et al. Boston bombings: a surgical view of lessons learned from combat casualty care and the applicability to Boston’s terrorist attack. J Craniofacial Surg. 2013;24:1061–1067. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
