

A transdiagnostic community-based mental health treatment for comorbid disorders: development and outcomes of a randomized controlled trial among Burmese refugees in Thailand
- PMID: 25386945
- PMCID: PMC4227644
- DOI: 10.1371/journal.pmed.1001757
A transdiagnostic community-based mental health treatment for comorbid disorders: development and outcomes of a randomized controlled trial among Burmese refugees in Thailand
Abstract
Background: Existing studies of mental health interventions in low-resource settings have employed highly structured interventions delivered by non-professionals that typically do not vary by client. Given high comorbidity among mental health problems and implementation challenges with scaling up multiple structured evidence-based treatments (EBTs), a transdiagnostic treatment could provide an additional option for approaching community-based treatment of mental health problems. Our objective was to test such an approach specifically designed for flexible treatments of varying and comorbid disorders among trauma survivors in a low-resource setting.
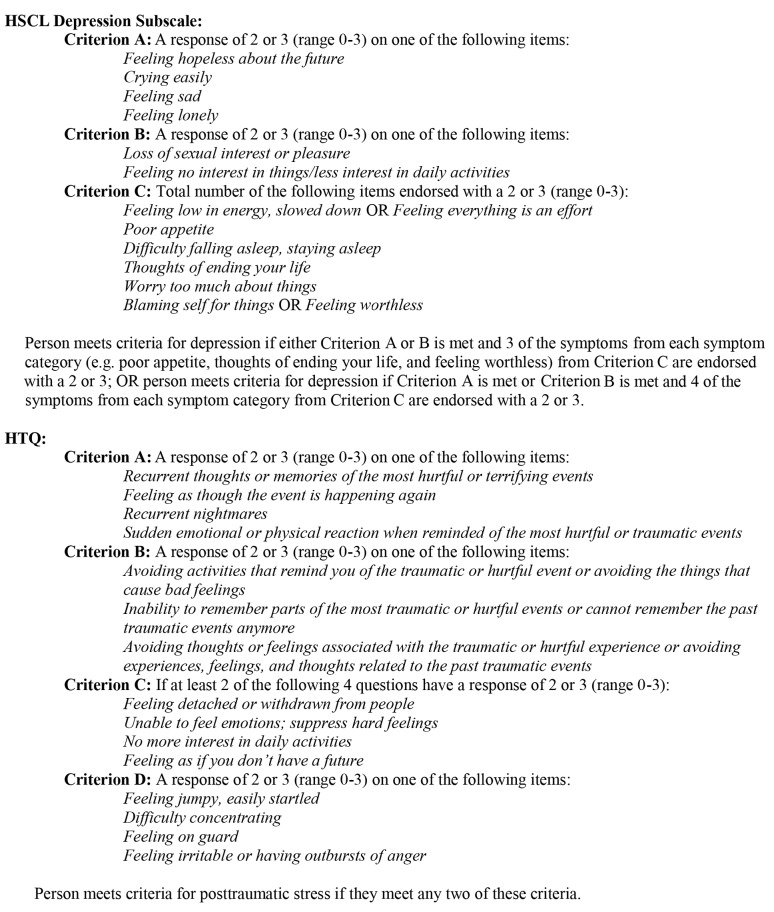
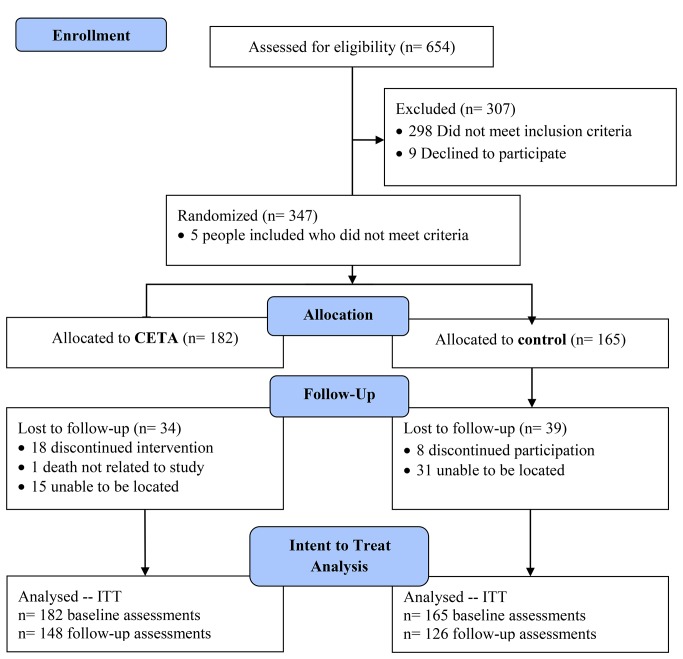
Methods and findings: We conducted a single-blinded, wait-list randomized controlled trial of a newly developed transdiagnostic psychotherapy, Common Elements Treatment Approach (CETA), for low-resource settings, compared with wait-list control (WLC). CETA was delivered by lay workers to Burmese survivors of imprisonment, torture, and related traumas, with flexibility based on client presentation. Eligible participants reported trauma exposure and met severity criteria for depression and/or posttraumatic stress (PTS). Participants were randomly assigned to CETA (n = 182) or WLC (n = 165). Outcomes were assessed by interviewers blinded to participant allocation using locally adapted standard measures of depression and PTS (primary outcomes) and functional impairment, anxiety symptoms, aggression, and alcohol use (secondary outcomes). Primary analysis was intent-to-treat (n = 347), including 73 participants lost to follow-up. CETA participants experienced significantly greater reductions of baseline symptoms across all outcomes with the exception of alcohol use (alcohol use analysis was confined to problem drinkers). The difference in mean change from pre-intervention to post-intervention between intervention and control groups was -0.49 (95% CI: -0.59, -0.40) for depression, -0.43 (95% CI: -0.51, -0.35) for PTS, -0.42 (95% CI: -0.58, -0.27) for functional impairment, -0.48 (95% CI: -0.61, -0.34) for anxiety, -0.24 (95% CI: -0.34, -0.15) for aggression, and -0.03 (95% CI: -0.44, 0.50) for alcohol use. This corresponds to a 77% reduction in mean baseline depression score among CETA participants compared to a 40% reduction among controls, with respective values for the other outcomes of 76% and 41% for anxiety, 75% and 37% for PTS, 67% and 22% for functional impairment, and 71% and 32% for aggression. Effect sizes (Cohen's d) were large for depression (d = 1.16) and PTS (d = 1.19); moderate for impaired function (d = 0.63), anxiety (d = 0.79), and aggression (d = 0.58); and none for alcohol use. There were no adverse events. Limitations of the study include the lack of long-term follow-up, non-blinding of service providers and participants, and no placebo or active comparison intervention.
Conclusions: CETA provided by lay counselors was highly effective across disorders among trauma survivors compared to WLCs. These results support the further development and testing of transdiagnostic approaches as possible treatment options alongside existing EBTs.
Trial registration: ClinicalTrials.gov NCT01459068 Please see later in the article for the Editors' Summary.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- McFarlane CA, Kaplan I (2012) Evidence-based psychological interventions for adult survivors of torture and trauma: a 30-year review. Transcult Psychiatry 49: 539–567. - PubMed
-
- Jordans MJ, Tol WA (2013) Mental health in humanitarian settings: shifting focus to care systems. Int Health 5: 9–10. - PubMed
-
- Bass JK, Annan J, McIvor Murray S, Kaysen D, Griffiths S, et al. (2013) Controlled trial of psychotherapy for Congolese survivors of sexual violence. N Engl J Med 368: 2182–2191. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
