

Pylorus-preserving pancreaticoduodenectomy (pp Whipple) versus pancreaticoduodenectomy (classic Whipple) for surgical treatment of periampullary and pancreatic carcinoma
- PMID: 25387229
- PMCID: PMC4356182
- DOI: 10.1002/14651858.CD006053.pub5
Pylorus-preserving pancreaticoduodenectomy (pp Whipple) versus pancreaticoduodenectomy (classic Whipple) for surgical treatment of periampullary and pancreatic carcinoma
Update in
-
Pylorus-preserving pancreaticoduodenectomy (pp Whipple) versus pancreaticoduodenectomy (classic Whipple) for surgical treatment of periampullary and pancreatic carcinoma.Cochrane Database Syst Rev. 2016 Feb 16;2(2):CD006053. doi: 10.1002/14651858.CD006053.pub6. Cochrane Database Syst Rev. 2016. PMID: 26905229 Free PMC article.
Abstract
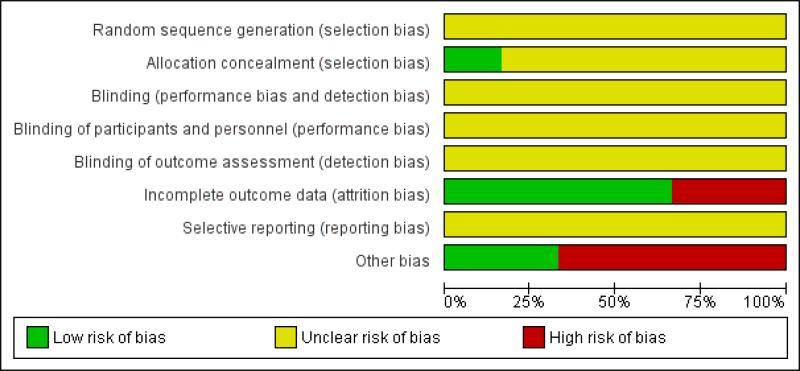
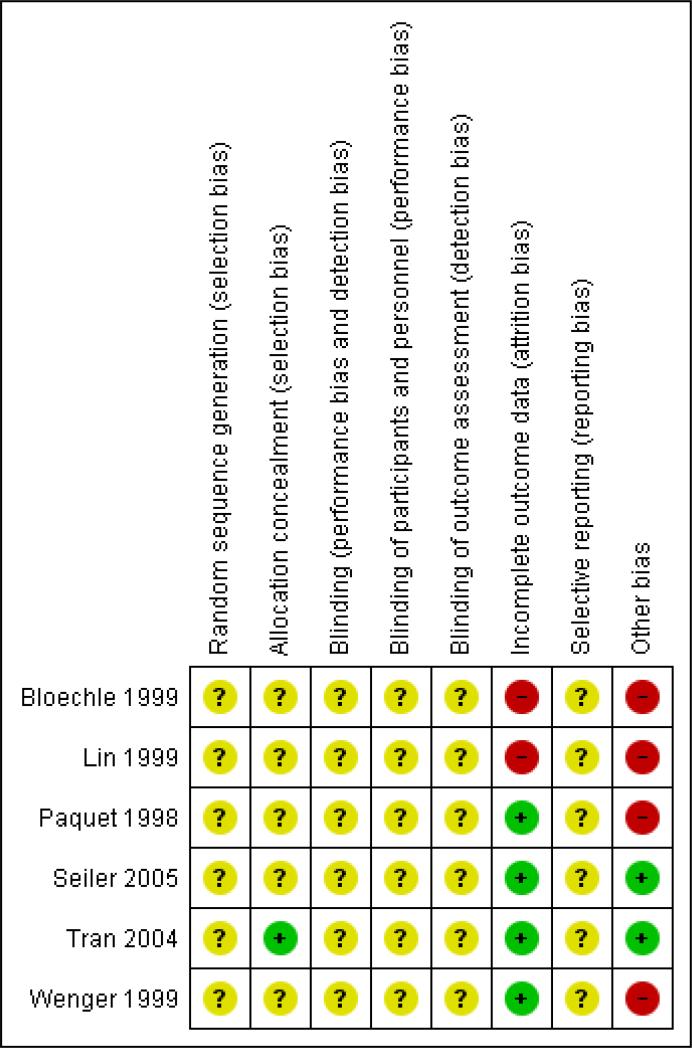
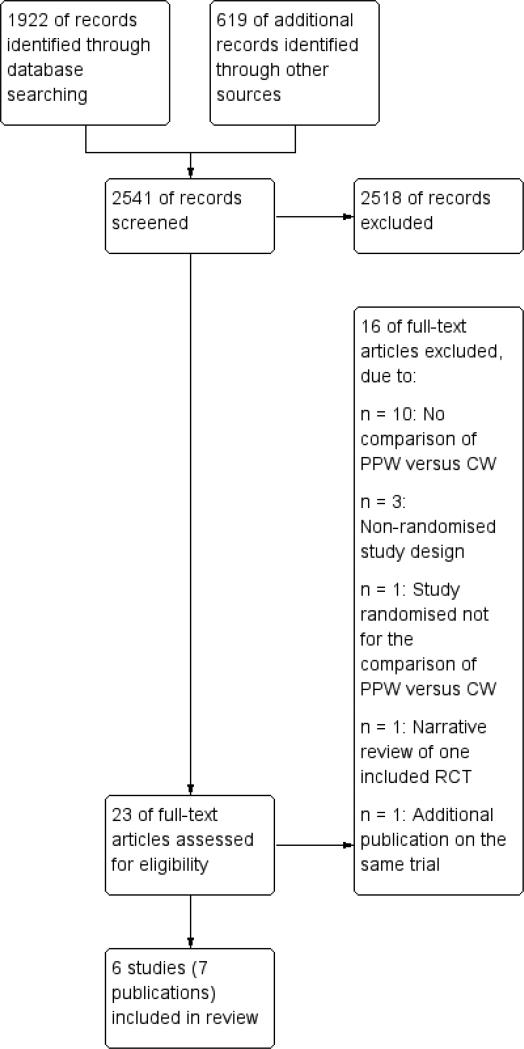
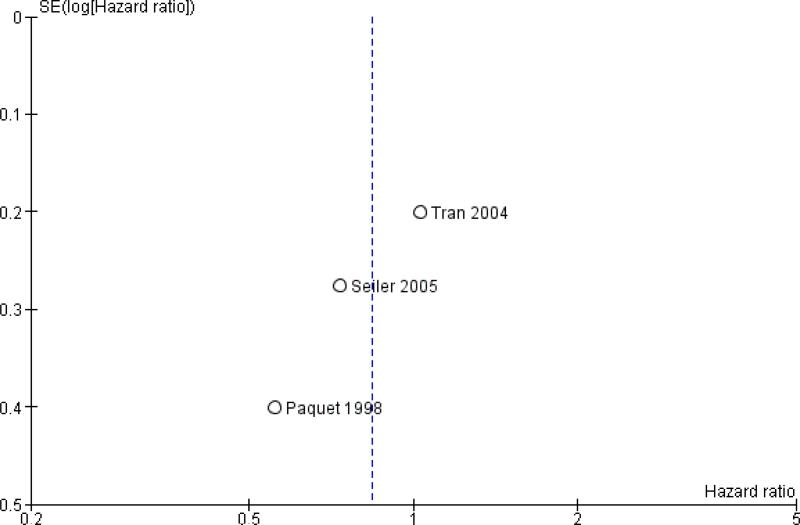
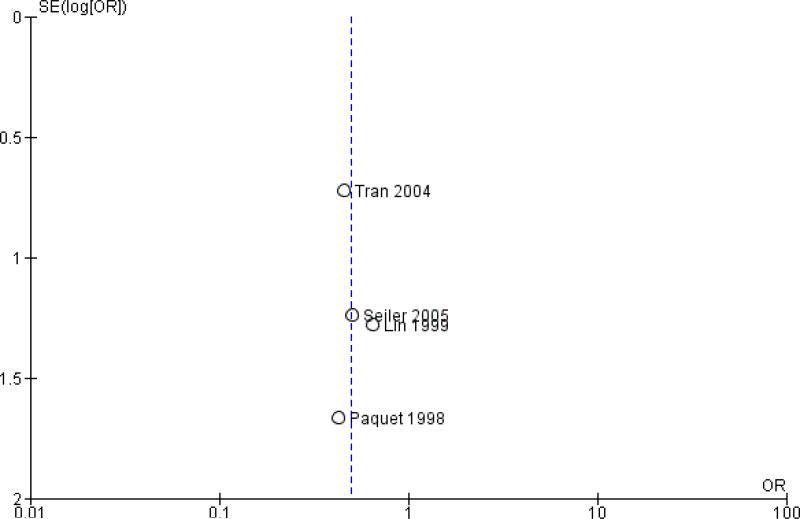
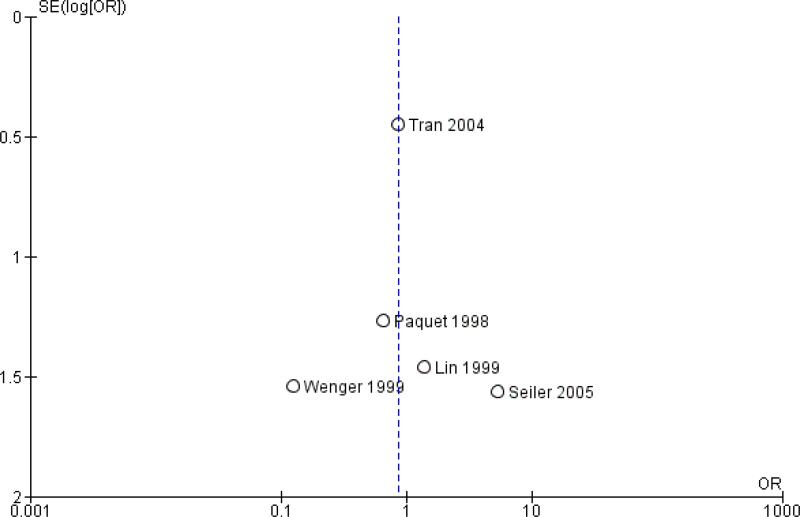
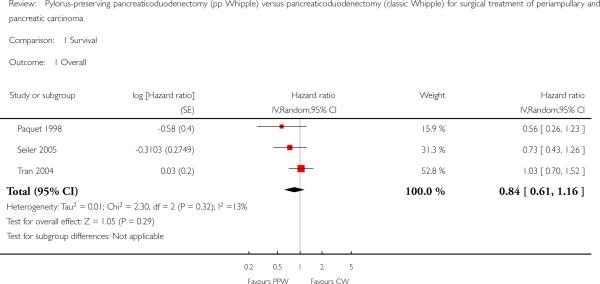
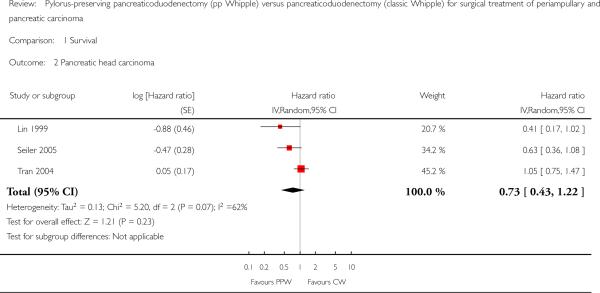
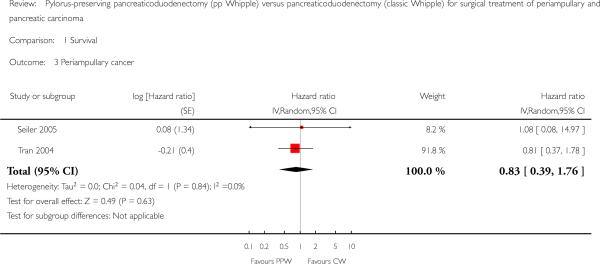
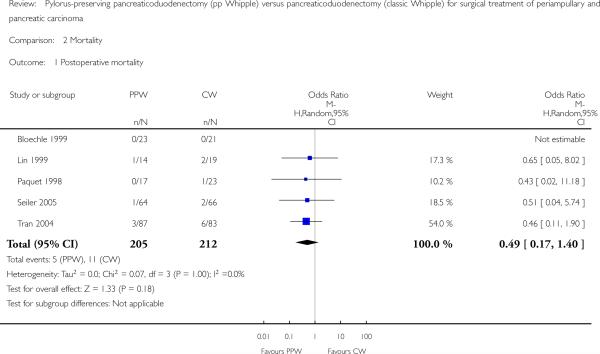
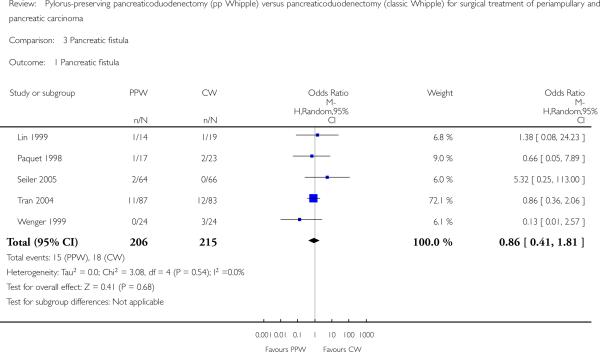
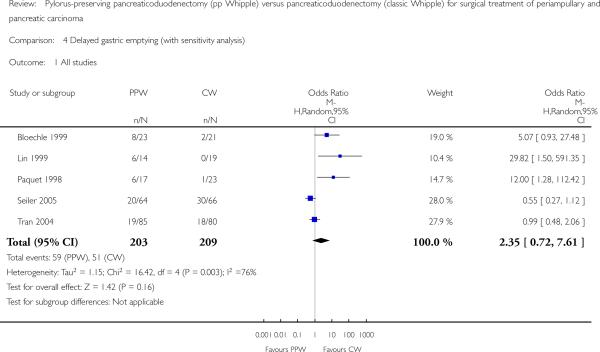
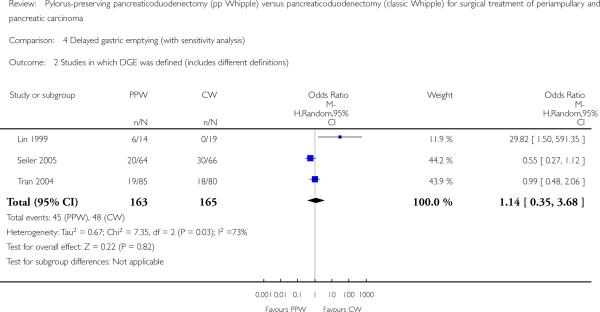
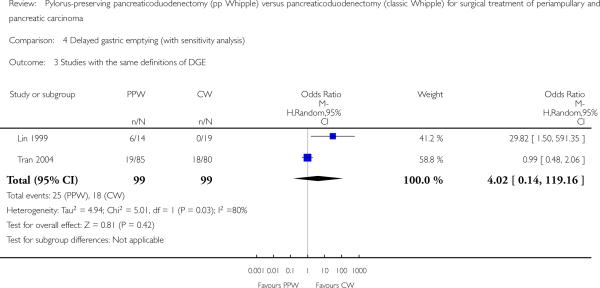
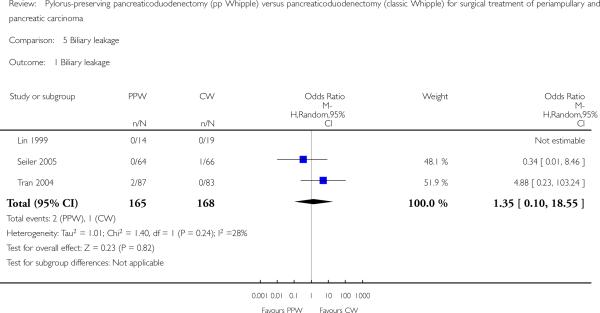
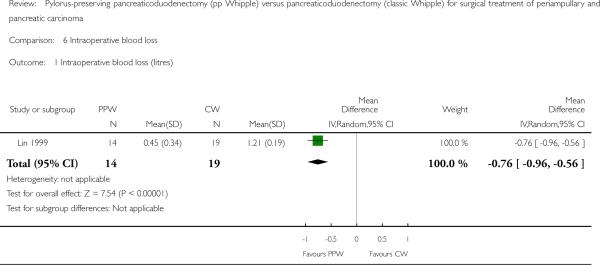
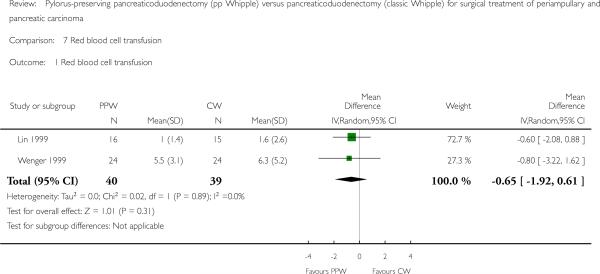
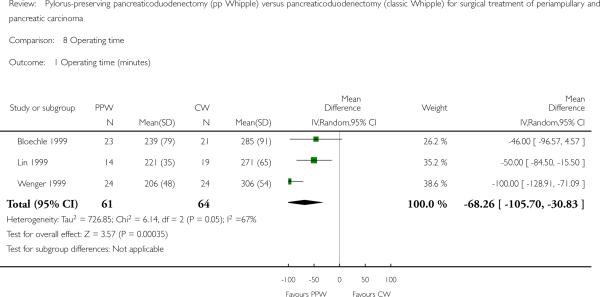
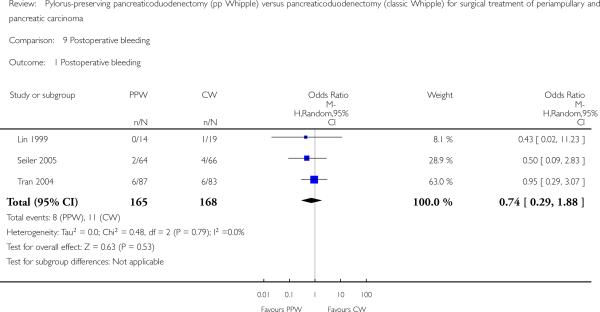
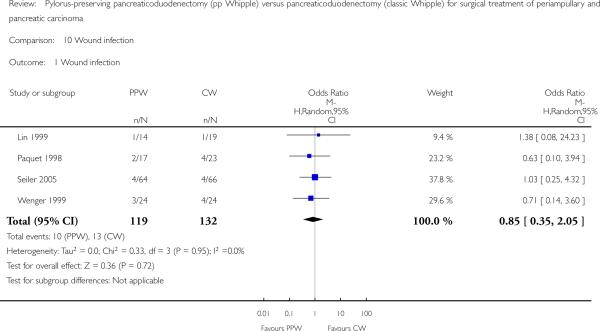
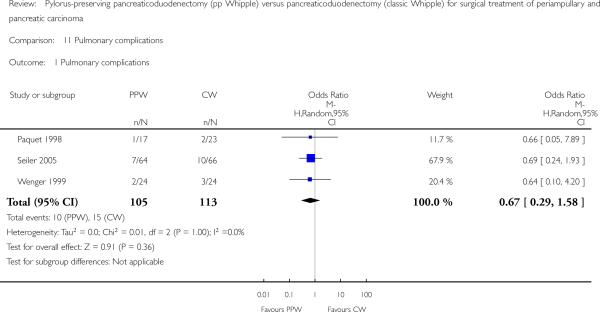
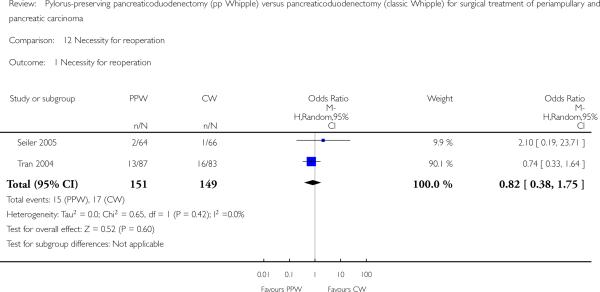
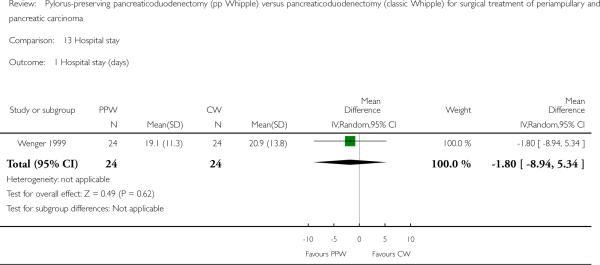
Background Pancreatic cancer is the fourth leading cause of cancer death for men and the fifth for women. The standard treatment for resectable tumours consists of a classic Whipple (CW) operation or a pylorus-preserving pancreaticoduodenectomy (PPW). It is unclear which of these procedures is more favourable in terms of survival, mortality, complications and quality of life.Objectives The objective of this systematic review is to compare the effectiveness of CW and PPW techniques for surgical treatment of cancer of the pancreatic head and the periampullary region.Search methods We conducted searches on 28 March 2006, 11 January 2011 and 9 January 2014 to identify all randomised controlled trials (RCTs),while applying no language restrictions. We searched the following electronic databases: the Cochrane Central Register of Controlled Trials (CENTRAL), the Cochrane Database of Systematic Reviews (CDSR) and the Database of Abstracts of Reviews of Effects(DARE) from The Cochrane Library (2013, Issue 4); MEDLINE (1946 to January 2014); and EMBASE (1980 to January 2014). We also searched abstracts from Digestive Disease Week and United European Gastroenterology Week (1995 to 2010). We identified no additional studies upon updating the systematic review in 2014.Selection criteria We considered RCTs comparing CW versus PPW to be eligible if they included study participants with periampullary or pancreatic carcinoma. Data collection and analysis Two review authors independently extracted data from the included studies. We used a random-effects model for pooling data. We compared binary outcomes using odds ratios (ORs), pooled continuous outcomes using mean differences (MDs) and used hazard ratios (HRs) for meta-analysis of survival. Two review authors independently evaluated the methodological quality and risk of bias of included studies according to the standards of The Cochrane Collaboration.Main results We included six RCTs with a total of 465 participants. Our critical appraisal revealed vast heterogeneity with respect to methodological quality and outcome parameters. In-hospital mortality (OR 0.49, 95% confidence interval (CI) 0.17 to 1.40; P value 0.18), overall survival (HR 0.84, 95% CI 0.61 to 1.16; P value 0.29) and morbidity showed no significant differences. However, we noted that operating time (MD -68.26 minutes, 95% CI -105.70 to -30.83; P value 0.0004) and intraoperative blood loss (MD -0.76 mL, 95%CI -0.96 to -0.56; P value < 0.00001) were significantly reduced in the PPW group. All significant results are associated with low quality of evidence as determined on the basis of GRADE (Grades of Recommendation, Assessment, Development and Evaluation) criteria.Authors' conclusions No evidence suggests relevant differences in mortality, morbidity and survival between the two operations. Given obvious clinical and methodological heterogeneity, future research must be undertaken to perform high-quality randomised controlled trials of complex surgical interventions on the basis of well-defined outcome parameters.
Figures
Update of
-
Pylorus-preserving pancreaticoduodenectomy (pp Whipple) versus pancreaticoduodenectomy (classic Whipple) for surgical treatment of periampullary and pancreatic carcinoma.Cochrane Database Syst Rev. 2011 May 11;(5):CD006053. doi: 10.1002/14651858.CD006053.pub4. Cochrane Database Syst Rev. 2011. Update in: Cochrane Database Syst Rev. 2014 Nov 11;(11):CD006053. doi: 10.1002/14651858.CD006053.pub5. PMID: 21563148 Updated.
References
-
- Bloechle C, Broering DC, Latuske C. Prospective randomized study to evaluate quality of life after partial pancreatoduodenectomy according to Whipple versus pylorus preserving pancreatoduodenectomy according to Longmire-Traverso for periampullary carcinoma. Deutsche Gesellschaft für Chirurgie. 1999;(Supplement 1):661–4. Forumband.
-
- Lin PW, Lin YJ. Prospective randomized comparison between pylorus-preserving and standard pancreaticoduodenectomy. British Journal of Surgery. 1999;86(5):603–7. - PubMed
-
- Lin PW, Shan YS, Lin YJ, Hung CJ. Pancreaticoduodenectomy for pancreatic head cancer: PPPD versus Whipple procedure. Hepatogastroenterology. 2005;52(65):1601–4. - PubMed
-
- Paquet K-J. Comparison of Whipple's pancreaticoduodenectomy with the pylorus-preserving pancreaticoduodenectomy-a prospectively controlled, randomized long-term trial [Vergleich der partiellen Duodenopankreatektomie (Whipple–Operation) mit der pyloruserhaltenden Zephaloduodenopankreatektomie-eine prospektive kontrollierte, randomisierte Langzeitstudie]. Chirurgische Gastroenterologie. 1998;14:54–8.
-
- Seiler CA, Wagner M, Bachmann T, Redaelli CA, Schmied B, Uhl W, et al. Randomized clinical trial of pylorus-preserving duodenopancreatectomy versus classical Whipple resection-long term results. British Journal of Surgery. 2005;92(5):547–56. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous