

Does use of pooled cohort risk score overestimate the use of statin?: a retrospective cohort study in a primary care setting
- PMID: 25388219
- PMCID: PMC4236445
- DOI: 10.1186/s12875-014-0172-y
Does use of pooled cohort risk score overestimate the use of statin?: a retrospective cohort study in a primary care setting
Abstract
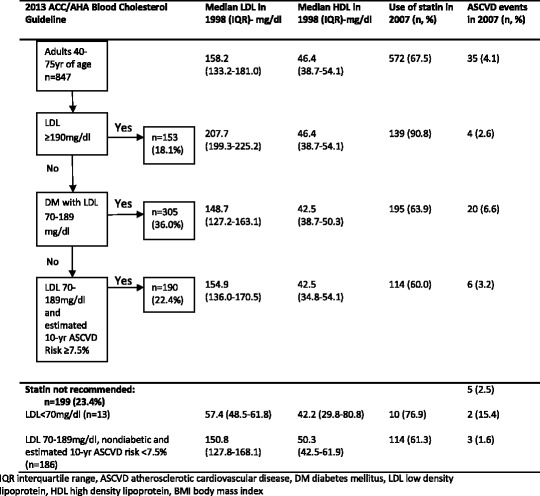
Background: Initiation of statin therapy as primary prevention particularly in those with mildly elevated cardiovascular disease risk factors is still being debated. The 2013 ACC/AHA blood cholesterol guideline recommends initiation of statin by estimating the 10-year atherosclerotic cardiovascular disease (ASCVD) risk using the new pooled cohort risk score. This paper examines the use of the pooled cohort risk score and compares it to actual use of statins in daily clinical practice in a primary care setting.
Methods: We examined the use of statins in a randomly selected sample of patients in a primary care clinic. The demographic data and cardiovascular risk parameters were captured from patient records in 1998. The pooled cohort risk score was calculated based on the parameters in 1998. The use of statins in 1998 and 2007, a 10-year interval, was recorded.
Results: A total of 847 patients were entered into the analysis. Mean age of the patients was 57.2 ± 8.4 years and 33.1% were male. The use of statins in 1998 was only 10.2% (n = 86) as compared to 67.5% (n = 572) in 2007. For patients with LDL 70-189 mg/dl and estimated 10-year ASCVD risk ≥7.5% (n = 190), 60% (n = 114) of patients were on statin therapy by 2007. There were 124 patients in whom statin therapy was not recommended according to ACC/AHA guideline but were actually receiving statin therapy.
Conclusions: An extra 40% of patients need to be treated with statin if the 2013 ACC/AHA blood cholesterol guideline is used. However the absolute number of patients who needed to be treated based on the ACC/AHA guideline is lower than the number of patients actually receiving it in a daily clinical practice. The pooled cohort risk score does not increase the absolute number of patients who are actually treated with statins. However these findings and the use of the pooled cohort risk score need to be validated further.
Figures
Similar articles
-
Does clinician-reported lipid guideline adoption translate to guideline-adherent care? An evaluation of the Patient and Provider Assessment of Lipid Management (PALM) registry.Am Heart J. 2018 Jun;200:118-124. doi: 10.1016/j.ahj.2018.03.011. Epub 2018 Mar 24. Am Heart J. 2018. PMID: 29898839 Free PMC article.
-
Initiation Patterns of Statins in the 2 Years After Release of the 2013 American College of Cardiology/American Heart Association (ACC/AHA) Cholesterol Management Guideline in a Large US Health Plan.J Am Heart Assoc. 2017 May 4;6(5):e005205. doi: 10.1161/JAHA.116.005205. J Am Heart Assoc. 2017. PMID: 28473405 Free PMC article.
-
Effect of 2013 ACC/AHA Blood Cholesterol Guidelines on Statin Treatment Patterns and Low-Density Lipoprotein Cholesterol in Atherosclerotic Cardiovascular Disease Patients.J Am Heart Assoc. 2017 Mar 17;6(3):e004909. doi: 10.1161/JAHA.116.004909. J Am Heart Assoc. 2017. PMID: 28314797 Free PMC article.
-
Systematic Review for the 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines.Circulation. 2019 Jun 18;139(25):e1144-e1161. doi: 10.1161/CIR.0000000000000626. Epub 2018 Nov 10. Circulation. 2019. PMID: 30586775
-
The new pooled cohort equations risk calculator.Can J Cardiol. 2015 May;31(5):613-9. doi: 10.1016/j.cjca.2015.02.001. Epub 2015 Feb 4. Can J Cardiol. 2015. PMID: 25843167 Review.
Cited by
-
Primary Prevention Using Cholesterol-Lowering Medications in Patients Meeting New Treatment Guidelines: A Retrospective Cohort Analysis.J Manag Care Spec Pharm. 2018 Nov;24(11):1078-1085. doi: 10.18553/jmcp.2018.24.11.1078. J Manag Care Spec Pharm. 2018. PMID: 30362921 Free PMC article.
-
Increases in statin eligibility to reduce cardiovascular risk according to the 2013 ACC/AHA cholesterol guidelines in the Africa Middle East region: a sub-analysis of the Africa Middle East Cardiovascular Epidemiological (ACE) study.BMC Cardiovasc Disord. 2019 Mar 15;19(1):61. doi: 10.1186/s12872-019-1034-2. BMC Cardiovasc Disord. 2019. PMID: 30876390 Free PMC article.
-
Validation of the pooled cohort risk score in an Asian population - a retrospective cohort study.BMC Cardiovasc Disord. 2014 Nov 20;14:163. doi: 10.1186/1471-2261-14-163. BMC Cardiovasc Disord. 2014. PMID: 25410585 Free PMC article.
-
An exploratory analysis of the metabolic syndrome and cardiovascular disease risk calculations in veterans with spinal cord injury and disorders.J Spinal Cord Med. 2025 Sep;48(5):875-883. doi: 10.1080/10790268.2024.2375888. Epub 2024 Jul 25. J Spinal Cord Med. 2025. PMID: 39051857 Free PMC article.
-
Awareness, knowledge and practice of dyslipidaemia management among postgraduate primary care trainees in Malaysia: a cross-sectional study.BMJ Open. 2017 Mar 1;7(3):e013573. doi: 10.1136/bmjopen-2016-013573. BMJ Open. 2017. PMID: 28249849 Free PMC article.
References
-
- Chia YC. Review of tools of cardiovascular disease risk stratification: interpretation, customization and application in clinical practice. Singapore Med J. 2011;52(2):116. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
