

Cross-sectional study of cytomegalovirus shedding and immunological markers among seropositive children and their mothers
- PMID: 25388365
- PMCID: PMC4236433
- DOI: 10.1186/s12879-014-0568-2
Cross-sectional study of cytomegalovirus shedding and immunological markers among seropositive children and their mothers
Abstract
Background: Congenital cytomegalovirus (CMV) is the leading infectious cause of birth defects in the United States. To better understand factors that may influence CMV transmission risk, we compared viral and immunological factors in healthy children and their mothers.
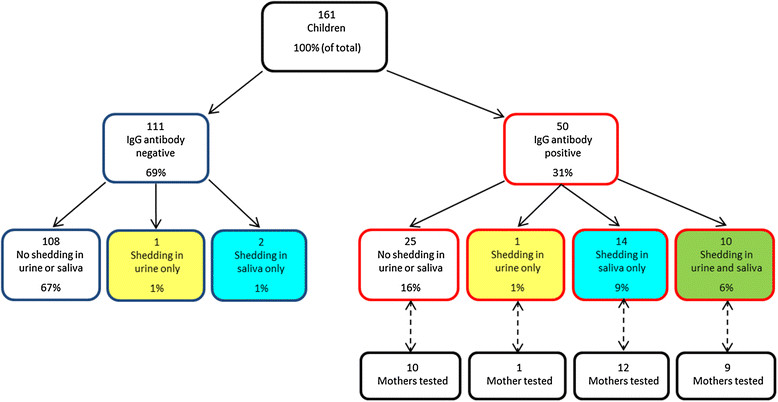
Methods: We screened for CMV IgG antibodies in a convenience sample of 161 children aged 0-47 months from the Atlanta, Georgia metropolitan area, along with 32 mothers of children who screened CMV-seropositive. We assessed CMV shedding via PCR using saliva collected with oral swabs (children and mothers) and urine collected from diapers using filter paper inserts (children only).
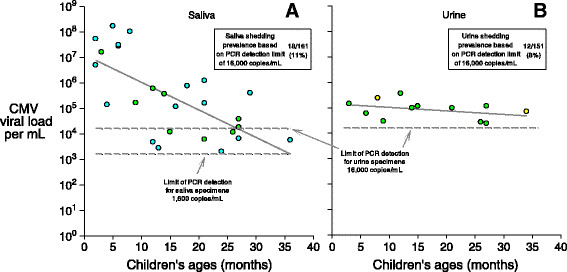
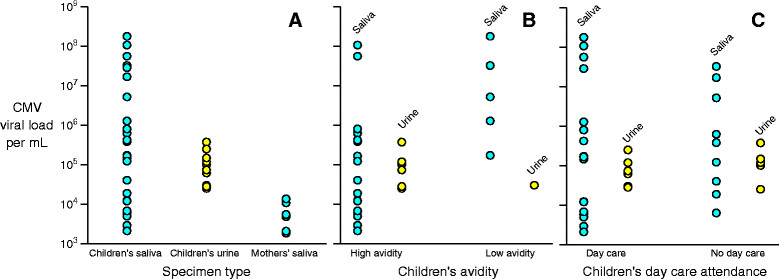
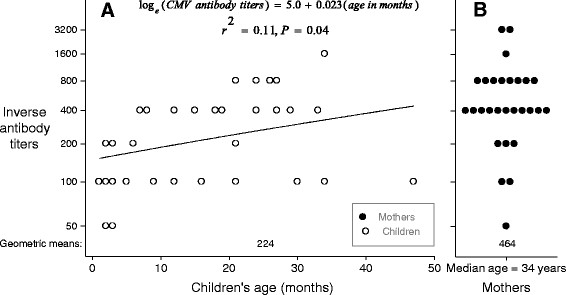
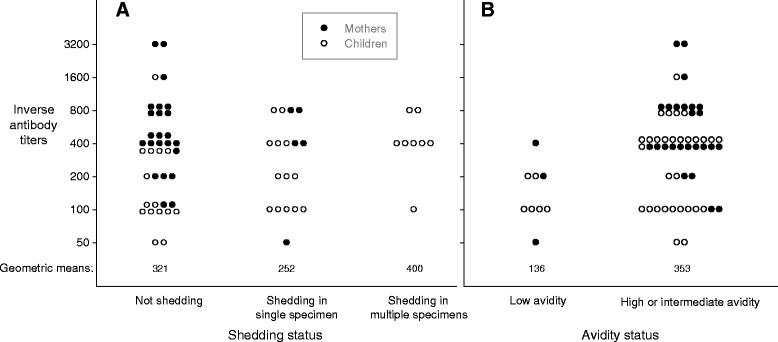
Results: CMV IgG was present in 31% (50/161) of the children. Half (25/50) of seropositive children were shedding in at least one fluid. The proportion of seropositive children who shed in saliva was 100% (8/8) among the 4-12 month-olds, 64% (9/14) among 13-24 month-olds, and 40% (6/15) among 25-47 month-olds (P for trend=0.003). Seropositive mothers had a lower proportion of saliva shedding (21% [6/29]) than children (P<0.001). Among children who were shedding CMV, viral loads in saliva were significantly higher in younger children (P <0.001); on average, the saliva viral load of infants (i.e., <12 months) was approximately 300 times that of two year-olds (i.e., 24-35 months). Median CMV viral loads were similar in children's saliva and urine but were 10-50 times higher (P<0.001) than the median viral load of the mothers' saliva. However, very high viral loads (> one million copies/mL) were only found in children's saliva (31% of those shedding); children's urine and mothers' saliva specimens all had fewer than 100,000 copies/mL. Low IgG avidity, a marker of primary infection, was associated with younger age (p=0.03), higher viral loads in saliva (p=0.02), and lower antibody titers (p=0.005).
Conclusions: Young CMV seropositive children, especially those less than one year-old may present high-risk CMV exposures to pregnant women, especially via saliva, though further research is needed to see if this finding can be generalized across racial or other demographic strata.
Figures

References
-
- Knowledge and practices of obstetricians and gynecologists regarding cytomegalovirus infection during pregnancy--United States, 2007. MMWR Morb Mortal Wkly Rep. 2008, 57 (3): 65-68. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
