

Transnasal Humidified Rapid-Insufflation Ventilatory Exchange (THRIVE): a physiological method of increasing apnoea time in patients with difficult airways
- PMID: 25388828
- PMCID: PMC4674986
- DOI: 10.1111/anae.12923
Transnasal Humidified Rapid-Insufflation Ventilatory Exchange (THRIVE): a physiological method of increasing apnoea time in patients with difficult airways
Abstract
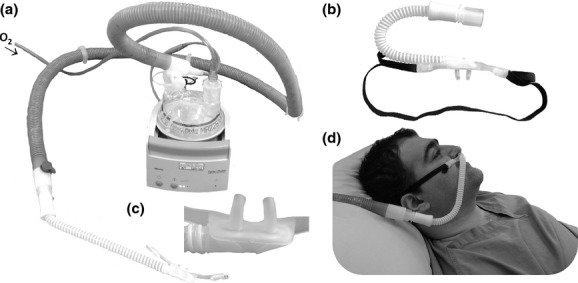
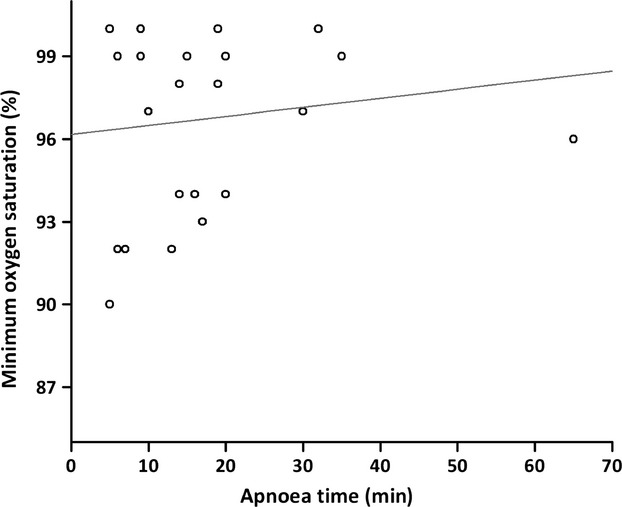
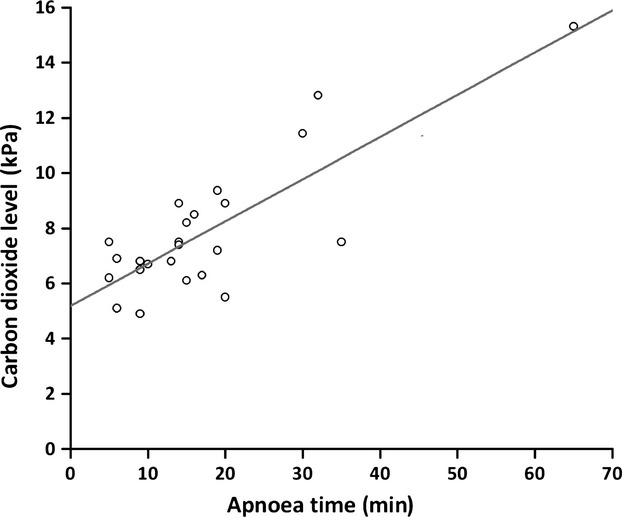
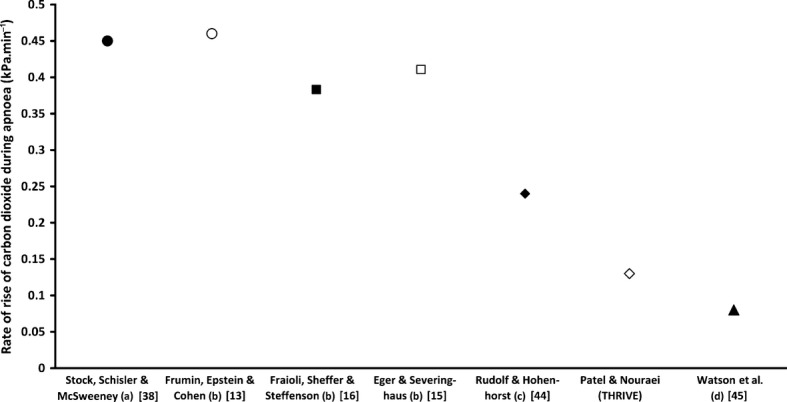
Emergency and difficult tracheal intubations are hazardous undertakings where successive laryngoscopy-hypoxaemia-re-oxygenation cycles can escalate to airway loss and the 'can't intubate, can't ventilate' scenario. Between 2013 and 2014, we extended the apnoea times of 25 patients with difficult airways who were undergoing general anaesthesia for hypopharyngeal or laryngotracheal surgery. This was achieved through continuous delivery of transnasal high-flow humidified oxygen, initially to provide pre-oxygenation, and continuing as post-oxygenation during intravenous induction of anaesthesia and neuromuscular blockade until a definitive airway was secured. Apnoea time commenced at administration of neuromuscular blockade and ended with commencement of jet ventilation, positive-pressure ventilation or recommencement of spontaneous ventilation. During this time, upper airway patency was maintained with jaw-thrust. Transnasal Humidified Rapid-Insufflation Ventilatory Exchange (THRIVE) was used in 15 males and 10 females. Mean (SD [range]) age at treatment was 49 (15 [25-81]) years. The median (IQR [range]) Mallampati grade was 3 (2-3 [2-4]) and direct laryngoscopy grade was 3 (3-3 [2-4]). There were 12 obese patients and nine patients were stridulous. The median (IQR [range]) apnoea time was 14 (9-19 [5-65]) min. No patient experienced arterial desaturation < 90%. Mean (SD [range]) post-apnoea end-tidal (and in four patients, arterial) carbon dioxide level was 7.8 (2.4 [4.9-15.3]) kPa. The rate of increase in end-tidal carbon dioxide was 0.15 kPa.min(-1) . We conclude that THRIVE combines the benefits of 'classical' apnoeic oxygenation with continuous positive airway pressure and gaseous exchange through flow-dependent deadspace flushing. It has the potential to transform the practice of anaesthesia by changing the nature of securing a definitive airway in emergency and difficult intubations from a pressured stop-start process to a smooth and unhurried undertaking.
© 2014 The Authors Anaesthesia published by John Wiley & Sons Ltd on behalf of Association of Anaesthetists of Great Britain and Ireland.
Figures
Comment in
-
Failure to THRIVE.Anaesthesia. 2015 Jun;70(6):752-3. doi: 10.1111/anae.13093. Anaesthesia. 2015. PMID: 25959182 No abstract available.
-
THRIVE--atelectasis, hypercarbia and consent.Anaesthesia. 2015 Jun;70(6):753-4. doi: 10.1111/anae.13118. Anaesthesia. 2015. PMID: 25959183 No abstract available.
-
Apnoeic oxygenation in noma patients.Anaesthesia. 2015 Jun;70(6):754-5. doi: 10.1111/anae.13111. Anaesthesia. 2015. PMID: 25959184 No abstract available.
-
Survive, then THRIVE.Anaesthesia. 2015 Jun;70(6):755. doi: 10.1111/anae.13119. Anaesthesia. 2015. PMID: 25959185 No abstract available.
-
A reply.Anaesthesia. 2015 Jun;70(6):755-6. doi: 10.1111/anae.13129. Anaesthesia. 2015. PMID: 25959186 No abstract available.
-
Oxygenation during difficult airway management.Anaesthesia. 2015 Nov;70(11):1330-1. doi: 10.1111/anae.13280. Anaesthesia. 2015. PMID: 26449304 No abstract available.
-
Carbon dioxide clearance during apnoea with high-flow nasal oxygen: epiphenomenon or a failure to THRIVE?Anaesthesia. 2020 May;75(5):580-582. doi: 10.1111/anae.14848. Epub 2019 Sep 6. Anaesthesia. 2020. PMID: 31489612 No abstract available.
-
Safe use of high flow nasal oxygen in apnoeic patients for laryngotracheal surgery: Adapting practice as technology evolves.Eur J Anaesthesiol. 2023 Nov 1;40(11):801-804. doi: 10.1097/EJA.0000000000001890. Epub 2023 Oct 11. Eur J Anaesthesiol. 2023. PMID: 37789752 No abstract available.
References
-
- Griesdale DEG, Bosma TL, Kurth T, Isac G, Chittock DR. Complications of endotracheal intubation in the critically ill. Intensive Care Medicine. 2008;34:1835–42. - PubMed
-
- Schulz CM, Endsley MR, Kochs EF, Gelb AW, Wagner KJ. Situation awareness in anesthesia: concept and research. Anesthesiology. 2013;118:729–42. - PubMed
-
- Cook TM, Woodall N, Frerk C. Major Complications of Airway Management in the United Kingdom: Report and Findings 4th National Audit of the Royal College of Anaesthetists and the Difficult Airway Society. London: National Patient Safety Agency; 2011. - PubMed
-
- Mort TC. The incidence and risk factors for cardiac arrest during emergency tracheal intubation: a justification for incorporating the ASA Guidelines in the remote location. Journal of Clinical Anesthesia. 2004;16:508–16. - PubMed
-
- Baraka AS, Taha SK, Aouad MT, El-Khatib MF, Kawkabani NI. Preoxygenation: comparison of maximal breathing and tidal volume breathing techniques. Anesthesiology. 1999;91:612–6. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
