

Early discharge after primary percutaneous coronary intervention: the added value of N-terminal pro-brain natriuretic peptide to the Zwolle Risk Score
- PMID: 25389283
- PMCID: PMC4338696
- DOI: 10.1161/JAHA.114.001089
Early discharge after primary percutaneous coronary intervention: the added value of N-terminal pro-brain natriuretic peptide to the Zwolle Risk Score
Abstract
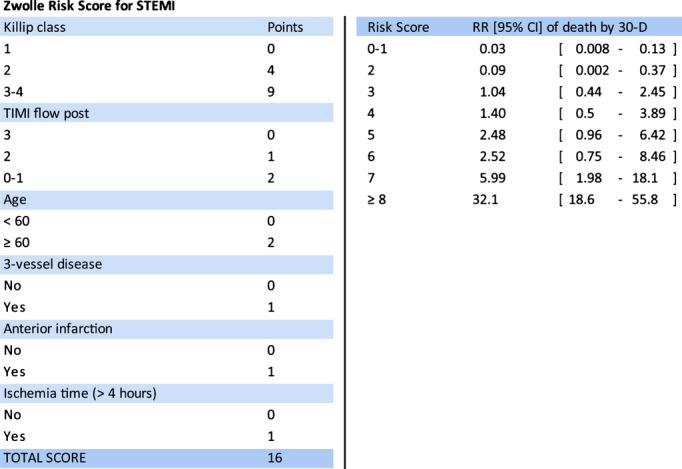
Background: The Zwolle Risk Score (ZRS) identifies ST-elevation myocardial infarction (STEMI) patients treated with primary percutaneous coronary intervention (PPCI) eligible for early discharge. We aimed to investigate whether baseline N-terminal pro-brain natriuretic peptide (NT-proBNP) is also able to identify these patients and could improve future risk strategies.
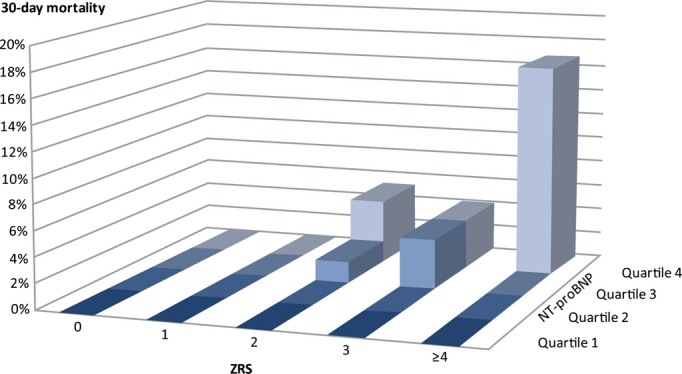
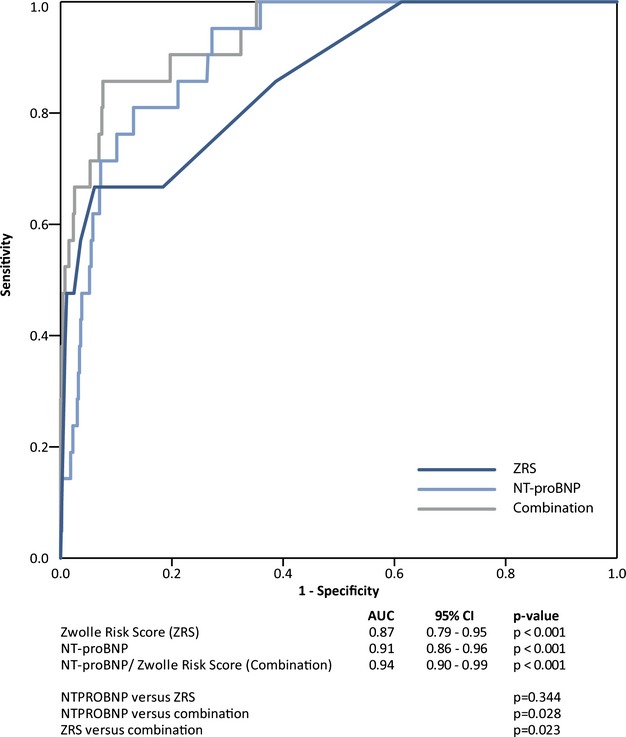
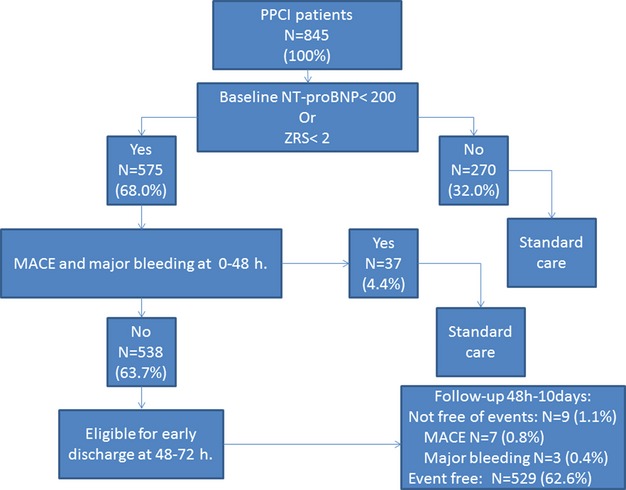
Methods and results: PPCI patients included in the Ongoing Tirofiban in Myocardial Infarction Evaluation (On-TIME) II study were candidates (N=861). We analyzed whether ZRS and baseline NT-proBNP predicted 30-day mortality and assessed the occurrence of major adverse cardiac events (MACEs) and major bleeding. Receiver operating characteristic curve analysis was used to assess discriminative accuracy for ZRS, NT-pro-BNP, and their combination. After multiple imputation, 845 patients were included. Both ZRS >3 (hazard ratio [HR]=9.42; P<0.001) and log NT-pro-BNP (HR=2.61; P<0.001) values were associated with 30-day mortality. On multivariate analysis, both the ZRS (HR=1.41; 95% confidence interval [CI]=1.27 to 1.56; P<0.001) and log NT-proBNP (HR=2.09; 95% CI=1.59 to 2.74; P<0.001) independently predicted death at 30 days. The area under the curve for 30-day mortality for combined ZRS/NT-proBNP was 0.94 (95% CI=0.90 to 0.99), with optimal predictive values of a ZRS ≥2 and a NT-proBNP value of ≥200 pg/mL. Using these cut-off values, 64% of the study population could be identified as very low risk with zero mortality at 30 days follow-up and low occurrence of MACEs and major bleeding between 48 hours and 10 days (1.3% and 0.6%, respectively).
Conclusion: Baseline NT-proBNP identifies a large group of low-risk patients who may be eligible for early (48- to 72-hour) discharge, whereas optimal predictive accuracy is reached by the combination of both baseline NT-proBNP and ZRS.
Keywords: NT‐proBNP; PCI; ST‐elevation myocardial infarction; Zwolle Risk Score; discharge; mortality; risk stratification.
© 2014 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
References
-
- Grines CL, Marsalese DL, Brodie B, Griffin J, Donohue B, Costantini CR, Balestrini C, Stone G, Wharton T, Esente P, Spain M, Moses J, Nobuyoshi M, Ayres M, Jones D, Sachs D, Mason D, Grines LL, O'Neill W. Safety and cost‐effectiveness of early discharge after primary angioplasty in low risk patients with acute myocardial infarction. PAMI‐II investigators. Primary Angioplasty in Myocardial Infarction. J Am Coll Cardiol. 1998; 5:967-972. - PubMed
-
- Branca G, Capodanno D, Capranzano P, Barbagallo R, Seminara D, Licciardello G, Tamburino C. Early discharge in acute myocardial infarction after clinical and angiographic risk assessment. J Cardiovasc Med (Hagerstown). 2008; 9:858-861. - PubMed
-
- Jirmar R, Widimsky P, Capek J, Hlinomaz O, Groch L. Next day discharge after successful primary angioplasty for acute ST elevation myocardial infarction. An open randomized study “Prague‐5.”. Int Heart J. 2008; 49:653-659. - PubMed
-
- Kotowycz MA, Cosman TL, Tartaglia C, Afzal R, Syal RP, Natarajan MK. Safety and feasibility of early hospital discharge in ST‐segment elevation myocardial infarction: a prospective and randomized trial in low risk primary percutaneous coronary intervention patients (The Safe‐Depart Trial). Am Heart J. 2010; 159:117.e1-117.e6. - PubMed
-
- Laarman GJ, Dirksen MT. Early discharge after primary percutaneous coronary intervention. Heart. 2010; 96:584-587. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
