

Application of veno-arterial-venous extracorporeal membrane oxygenation in differential hypoxia
- PMID: 25389467
- PMCID: PMC4226883
- DOI: 10.1186/2049-6958-9-55
Application of veno-arterial-venous extracorporeal membrane oxygenation in differential hypoxia
Abstract
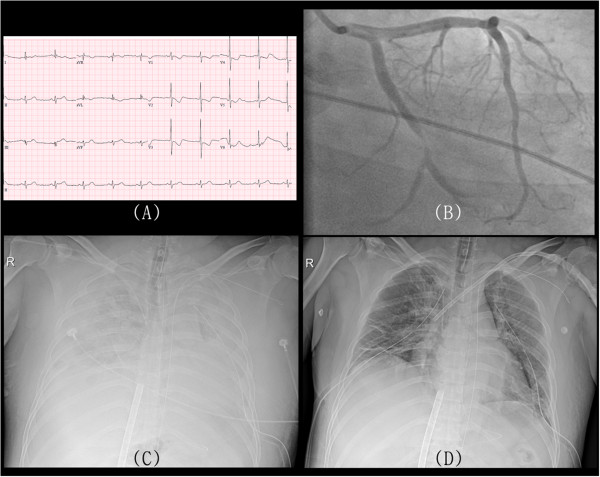
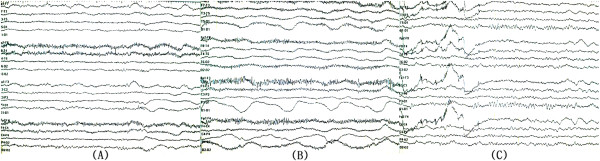
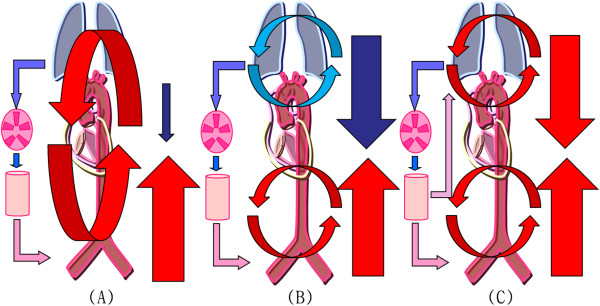
Veno-arterial extracorporeal membrane oxygenation (ECMO) through the femoral vein and artery may cause differential hypoxia, i.e., lower PaO2 in the upper body than in the lower body, because of normal cardiac output with severe impairment of pulmonary function. Hereby, we report the diagnosis and the treatment of differential hypoxia caused by veno-arterial ECMO. A 39-year-old man received cardiopulmonary resuscitation from a cardiac arrest due to acute myocardial infarction. Even after more than 30 min of resuscitation, spontaneous circulation had not resumed. Next, we performed veno-arterial ECMO through the femoral artery and vein, and the patient recovered consciousness on the second day of ECMO. On day 5 of ECMO, he lost consciousness again and presented a generalized tonic-clonic seizure, and an electroencephalogram showed delta waves suggesting diffuse cerebral cortical dysfunction. While an echocardiogram revealed improvements in myocardial function, a follow up chest radiograph showed increasing massive parenchymal infiltrations, and gas analysis of blood from the right radial artery revealed severe hypoxemia. These findings indicated a definite diagnosis of differential hypoxia, and therefore, we inserted a 17-Fr cannula into the left subclavian vein as a return cannula. The patient's consciousness and pulmonary infiltrations were improved 2 days after veno-arterial-venous ECMO, and the electroencephalogram showed normal findings. To our knowledge, this is the first report of successful clinical management of differential hypoxia. We suggest that veno-arterial-venous ECMO could be the treatment of choice for differential hypoxia resulting from veno-arterial ECMO.
Keywords: Brain; Extracorporeal membrane oxygenation; Lungs; Pulmonary function.
Figures
References
-
- Peek GJ, Mugford M, Tiruvoipati R, Wilson A, Allen E, Thalanany MM, Hibbert CL, Truesdale A, Clemens F, Cooper N, Firmin RK, Elbourne D. Efficacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR): a multicenter randomised controlled trial. Lancet. 2009;374:1351–1363. doi: 10.1016/S0140-6736(09)61069-2. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
