

Predicting suicides after psychiatric hospitalization in US Army soldiers: the Army Study To Assess Risk and rEsilience in Servicemembers (Army STARRS)
- PMID: 25390793
- PMCID: PMC4286426
- DOI: 10.1001/jamapsychiatry.2014.1754
Predicting suicides after psychiatric hospitalization in US Army soldiers: the Army Study To Assess Risk and rEsilience in Servicemembers (Army STARRS)
Abstract
Importance: The US Army experienced a sharp increase in soldier suicides beginning in 2004. Administrative data reveal that among those at highest risk are soldiers in the 12 months after inpatient treatment of a psychiatric disorder.
Objective: To develop an actuarial risk algorithm predicting suicide in the 12 months after US Army soldier inpatient treatment of a psychiatric disorder to target expanded posthospitalization care.
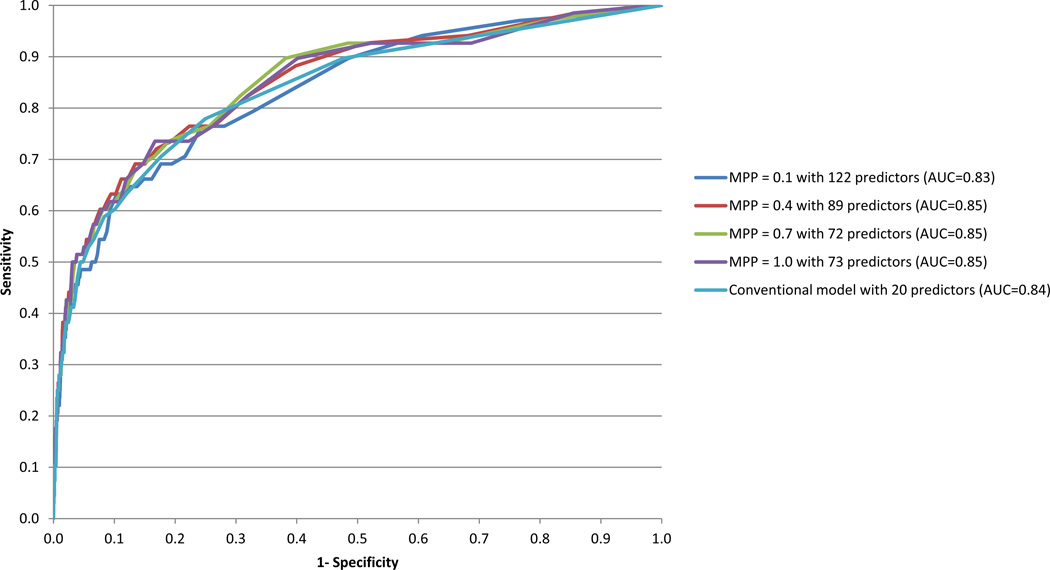
Design, setting, and participants: There were 53,769 hospitalizations of active duty soldiers from January 1, 2004, through December 31, 2009, with International Classification of Diseases, Ninth Revision, Clinical Modification psychiatric admission diagnoses. Administrative data available before hospital discharge abstracted from a wide range of data systems (sociodemographic, US Army career, criminal justice, and medical or pharmacy) were used to predict suicides in the subsequent 12 months using machine learning methods (regression trees and penalized regressions) designed to evaluate cross-validated linear, nonlinear, and interactive predictive associations.
Main outcomes and measures: Suicides of soldiers hospitalized with psychiatric disorders in the 12 months after hospital discharge.
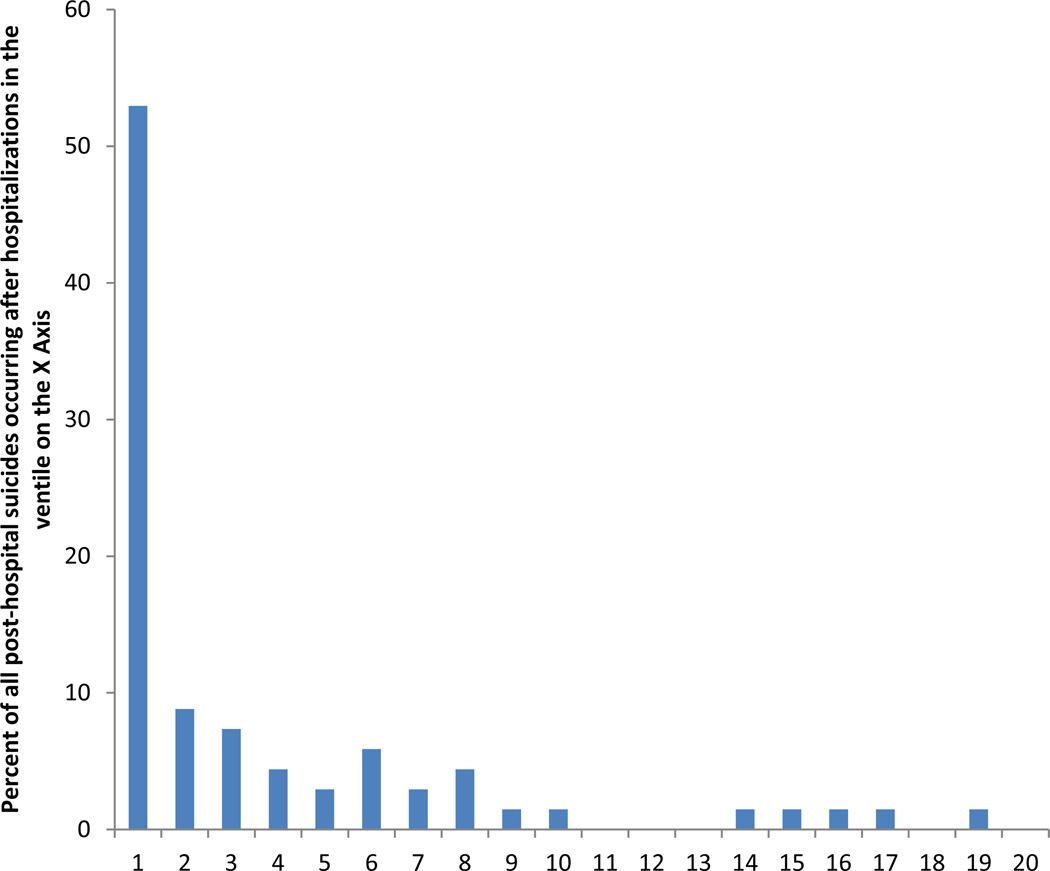
Results: Sixty-eight soldiers died by suicide within 12 months of hospital discharge (12.0% of all US Army suicides), equivalent to 263.9 suicides per 100,000 person-years compared with 18.5 suicides per 100,000 person-years in the total US Army. The strongest predictors included sociodemographics (male sex [odds ratio (OR), 7.9; 95% CI, 1.9-32.6] and late age of enlistment [OR, 1.9; 95% CI, 1.0-3.5]), criminal offenses (verbal violence [OR, 2.2; 95% CI, 1.2-4.0] and weapons possession [OR, 5.6; 95% CI, 1.7-18.3]), prior suicidality [OR, 2.9; 95% CI, 1.7-4.9], aspects of prior psychiatric inpatient and outpatient treatment (eg, number of antidepressant prescriptions filled in the past 12 months [OR, 1.3; 95% CI, 1.1-1.7]), and disorders diagnosed during the focal hospitalizations (eg, nonaffective psychosis [OR, 2.9; 95% CI, 1.2-7.0]). A total of 52.9% of posthospitalization suicides occurred after the 5% of hospitalizations with highest predicted suicide risk (3824.1 suicides per 100,000 person-years). These highest-risk hospitalizations also accounted for significantly elevated proportions of several other adverse posthospitalization outcomes (unintentional injury deaths, suicide attempts, and subsequent hospitalizations).
Conclusions and relevance: The high concentration of risk of suicide and other adverse outcomes might justify targeting expanded posthospitalization interventions to soldiers classified as having highest posthospitalization suicide risk, although final determination requires careful consideration of intervention costs, comparative effectiveness, and possible adverse effects.
Figures
References
-
- Armed Forces Health Surveillance Center. Deaths by suicide while on active duty, active and reserve components, U.S. Armed Forces, 1998–2011. Med Surveill Monthly Rep. 2012;19(6):7–10. - PubMed
-
- Zamorski MA. Suicide prevention in military organizations. Int Rev Psychiatry. 2011;23(2):173–180. - PubMed
-
- Luxton DD, Trofimovich L, Clark LL. Suicide risk among US Service members after psychiatric hospitalization, 2001–2011. Psychiatr Serv. 2013;64(7):626–629. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
