

Right ventricular function in heart failure with preserved ejection fraction: a community-based study
- PMID: 25391518
- PMCID: PMC4276536
- DOI: 10.1161/CIRCULATIONAHA.113.008461
Right ventricular function in heart failure with preserved ejection fraction: a community-based study
Erratum in
-
Correction.Circulation. 2015 Apr 28;131(17):e424. doi: 10.1161/CIR.0000000000000202. Circulation. 2015. PMID: 25918046 No abstract available.
Abstract
Background: The prevalence and clinical significance of right ventricular (RV) systolic dysfunction (RVD) in patients with heart failure and preserved ejection fraction (HFpEF) are not well characterized.
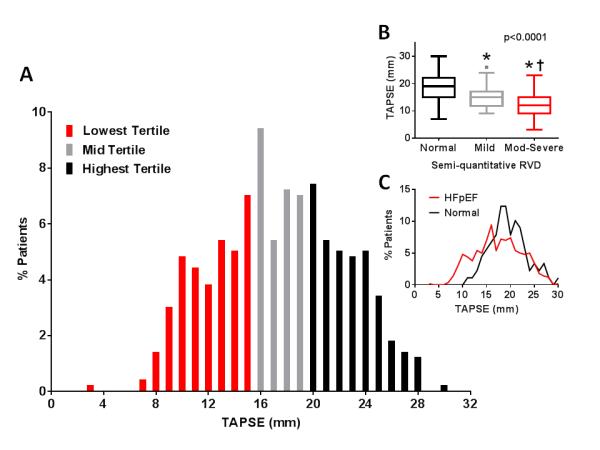
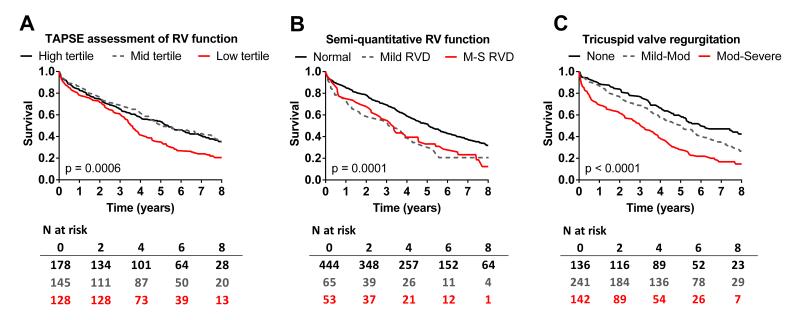
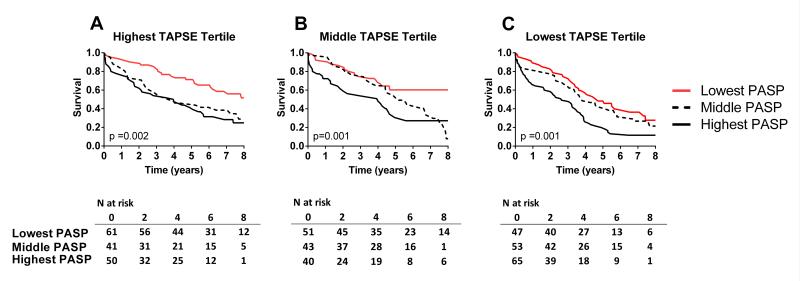
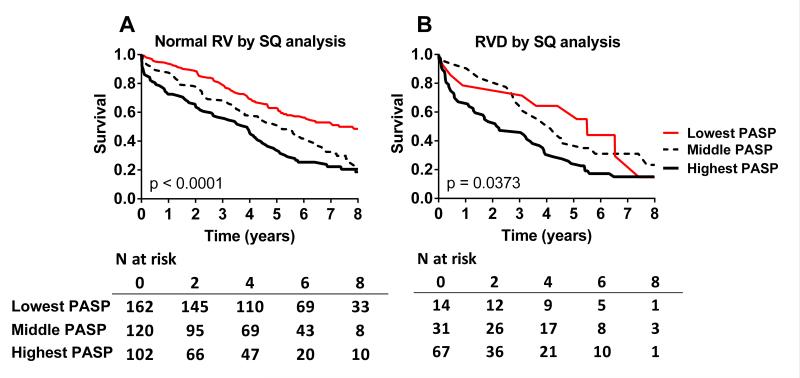
Methods and results: Consecutive, prospectively identified HFpEF (Framingham HF criteria, ejection fraction ≥50%) patients (n=562) from Olmsted County, Minnesota, underwent echocardiography at HF diagnosis and follow-up for cause-specific mortality and HF hospitalization. RV function was categorized by tertiles of tricuspid annular plane systolic excursion and by semiquantitative (normal, mild RVD, or moderate to severe RVD) 2-dimensional assessment. Whether RVD was defined by semiquantitative assessment or tricuspid annular plane systolic excursion ≤15 mm, HFpEF patients with RVD were more likely to have atrial fibrillation, pacemakers, and chronic diuretic therapy. At echocardiography, patients with RVD had slightly lower left ventricular ejection fraction, worse diastolic dysfunction, lower blood pressure and cardiac output, higher pulmonary artery systolic pressure, and more severe RV enlargement and tricuspid valve regurgitation. After adjustment for age, sex, pulmonary artery systolic pressure, and comorbidities, the presence of any RVD by semiquantitative assessment was associated with higher all-cause (hazard ratio=1.35; 95% confidence interval, 1.03-1.77; P=0.03) and cardiovascular (hazard ratio=1.85; 95% confidence interval, 1.20-2.80; P=0.006) mortality and higher first (hazard ratio=1.99; 95% confidence interval, 1.35-2.90; P=0.0006) and multiple (hazard ratio=1.81; 95% confidence interval, 1.18-2.78; P=0.007) HF hospitalization rates. RVD defined by tricuspid annular plane systolic excursion values showed similar but weaker associations with mortality and HF hospitalizations.
Conclusions: In the community, RVD is common in HFpEF patients, is associated with clinical and echocardiographic evidence of more advanced HF, and is predictive of poorer outcomes.
Keywords: diastole; heart failure; hypertension, pulmonary; ventricular dysfunction, right.
© 2014 American Heart Association, Inc.
Figures
Comment in
-
It is time to look at heart failure with preserved ejection fraction from the right side.Circulation. 2014 Dec 23;130(25):2272-7. doi: 10.1161/CIRCULATIONAHA.114.013536. Epub 2014 Nov 12. Circulation. 2014. PMID: 25391521 Free PMC article. No abstract available.
-
Letter by Guazzi regarding article, "right ventricular function in heart failure with preserved ejection fraction: a community-based study".Circulation. 2015 Sep 29;132(13):e160. doi: 10.1161/CIRCULATIONAHA.114.014332. Circulation. 2015. PMID: 26416633 No abstract available.
-
Response to letter regarding article, "right ventricular function in heart failure with preserved ejection fraction: a community-based study".Circulation. 2015 Sep 29;132(13):e161. doi: 10.1161/CIRCULATIONAHA.115.016481. Circulation. 2015. PMID: 26416634 No abstract available.
References
-
- Iglesias-Garriz I, Olalla-Gomez C, Garrote C, Lopez-Benito M, Martin J, Alonso D, Rodriguez MA. Contribution of right ventricular dysfunction to heart failure mortality: A meta-analysis. Rev Cardiovasc Med. 2012;13:e62–69. - PubMed
-
- Weiner BH, Alpert JS, Dalen JE, Ockene IS. Response of the right ventricle to exercise in patients with chronic heart disease. Am Heart J. 1983;105:386–393. - PubMed
-
- Baker BJ, Wilen MM, Boyd CM, Dinh H, Franciosa JA. Relation of right ventricular ejection fraction to exercise capacity in chronic left ventricular failure. Am J Cardiol. 1984;54:596–599. - PubMed
-
- Di Salvo TG, Mathier M, Semigran MJ, Dec GW. Preserved right ventricular ejection fraction predicts exercise capacity and survival in advanced heart failure. J Am Coll Cardiol. 1995;25:1143–1153. - PubMed
-
- Gorcsan J, 3rd, Murali S, Counihan PJ, Mandarino WA, Kormos RL. Right ventricular performance and contractile reserve in patients with severe heart failure. Assessment by pressure-area relations and association with outcome. Circulation. 1996;94:3190–3197. - PubMed
Publication types
MeSH terms
Grants and funding
- R01 HL72435/HL/NHLBI NIH HHS/United States
- R01 HL055502/HL/NHLBI NIH HHS/United States
- U01HL 084907/HL/NHLBI NIH HHS/United States
- HL72435/HL/NHLBI NIH HHS/United States
- T32-HL007111/HL/NHLBI NIH HHS/United States
- P01HL 76611/HL/NHLBI NIH HHS/United States
- HL 55502/HL/NHLBI NIH HHS/United States
- T32 HL007111/HL/NHLBI NIH HHS/United States
- R01 HL072435/HL/NHLBI NIH HHS/United States
- R01 HL105418/HL/NHLBI NIH HHS/United States
- U01 HL084907/HL/NHLBI NIH HHS/United States
- UL1 TR000135/TR/NCATS NIH HHS/United States
- U01 HL 0084907/HL/NHLBI NIH HHS/United States
- U10 HL110262/HL/NHLBI NIH HHS/United States
- U10 HL 110262/HL/NHLBI NIH HHS/United States
- P01 HL076611/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
