

Updated hysterectomy surveillance and factors associated with minimally invasive hysterectomy
- PMID: 25392662
- PMCID: PMC4208898
- DOI: 10.4293/JSLS.2014.00096
Updated hysterectomy surveillance and factors associated with minimally invasive hysterectomy
Abstract
Background and objectives: The goal of this study is to obtain updated surveillance statistics for hysterectomy procedures in the United States and identify factors associated with undergoing a minimally invasive approach to hysterectomy.
Methods: A cross-sectional analysis of the 2009 United States Nationwide Inpatient Sample was performed. Subjects included all women aged 18 years or older who underwent hysterectomy of any type. Logistic regression and multivariate analyses were performed to assess the proportion of hysterectomies performed by various routes, as well as factors associated with undergoing minimally invasive surgery (laparoscopic, vaginal, or robotic).
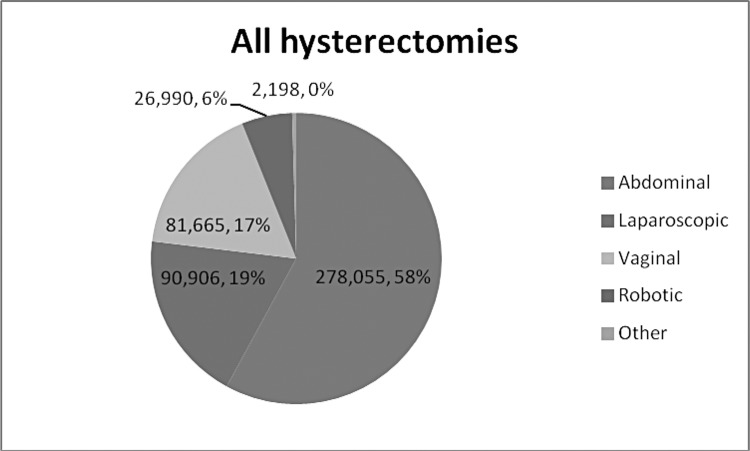
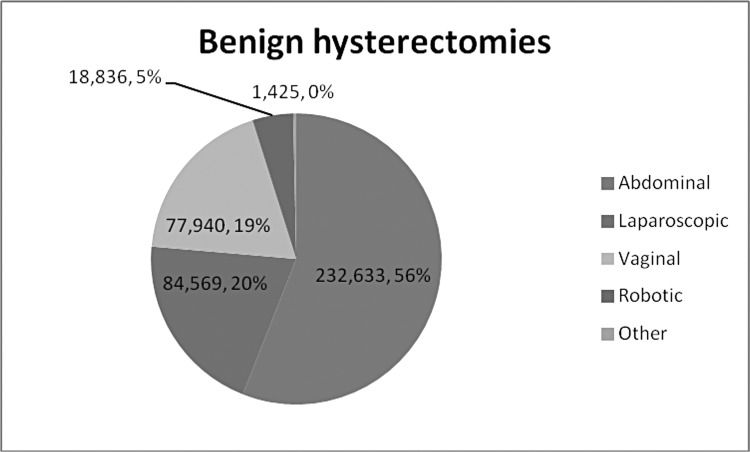
Results: A total of 479,814 hysterectomies were performed in the United States in 2009, 86.6% of which were performed for benign indications. Among the hysterectomies performed for benign indications, 56% were completed abdominally, 20.4% were performed laparoscopically, 18.8% were performed vaginally, and 4.5% were performed with robotic assistance. Factors associated with decreased odds of a minimally invasive hysterectomy included the following: minority race (P<.0001), fibroids (P<.0001), concomitant adnexal surgery (P<.0001), self-pay (P=.01) or Medicaid as insurer (P<.0001), and increased severity of illness (P<.0001). Factors associated with increased odds of a minimally invasive hysterectomy included the following: age>50 years (P<.0001), prolapse or menstrual disorder (P<.0001), median household income of $48,000-$62,999 (P=.007) or ≥$63,000 (P=.009), and location in the West (P=.02). A length of stay>1 day was most common in abdominal hysterectomy cases (96.1%), although total mean charges were highest for robotic cases ($38,161).
Conclusion: The US hysterectomy incidence in 2009 decreased from prior years' reports, with an increasing frequency of laparoscopic and robotic approaches. Racial and socioeconomic factors influenced hysterectomy mode.
Keywords: Hysterectomy; Socioeconomic; Surveillance.
Figures
References
-
- ACOG Committee Opinion No. 444: choosing the route of hysterectomy for benign disease. Obstet Gynecol. 2009;114(5):1156–1158 - PubMed
-
- AAGL Advancing Minimally Invasive Gynecology Worldwide. AAGL position statement: route of hysterectomy to treat benign uterine disease. J Minim Invasive Gynecol. 2011;18(1):1–3 - PubMed
-
- Nieboer TE, Johnson N, Lethaby A, et al. Surgical approach to hysterectomy for benign gynaecological disease. Cochrane Database Syst Rev. 2009;(3):CD003677. - PubMed
-
- Wu JM, Wechter ME, Geller EJ, Nguyen TV, Visco AG. Hysterectomy rates in the United States, 2003. Obstet Gynecol. 2007;110(5):1091–1095 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical