

Exhaled air dispersion during noninvasive ventilation via helmets and a total facemask
- PMID: 25392954
- PMCID: PMC7094250
- DOI: 10.1378/chest.14-1934
Exhaled air dispersion during noninvasive ventilation via helmets and a total facemask
Abstract
Background: Noninvasive ventilation (NIV) via helmet or total facemask is an option for managing patients with respiratory infections in respiratory failure. However, the risk of nosocomial infection is unknown.
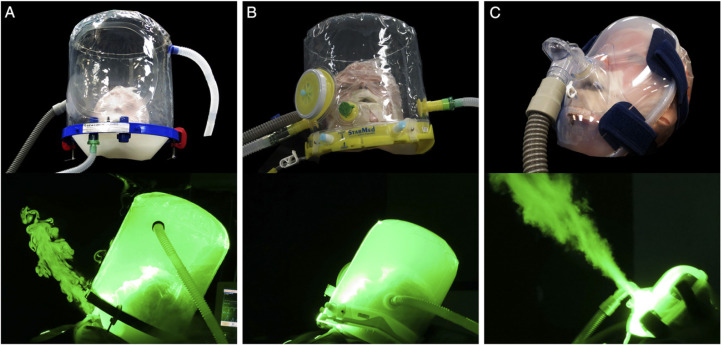
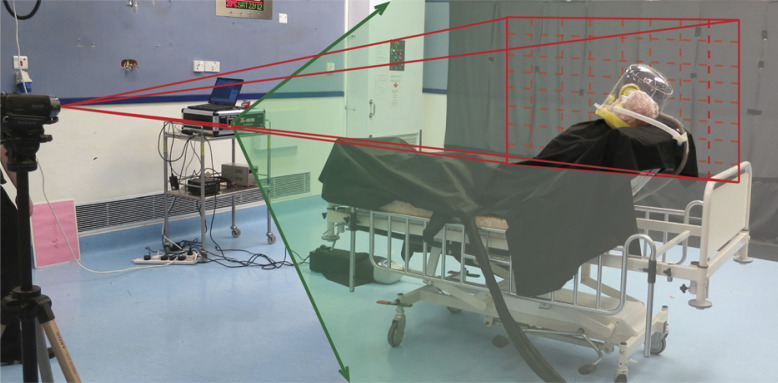
Methods: We examined exhaled air dispersion during NIV using a human patient simulator reclined at 45° in a negative pressure room with 12 air changes/h by two different helmets via a ventilator and a total facemask via a bilevel positive airway pressure device. Exhaled air was marked by intrapulmonary smoke particles, illuminated by laser light sheet, and captured by a video camera for data analysis. Significant exposure was defined as where there was ≥ 20% of normalized smoke concentration.
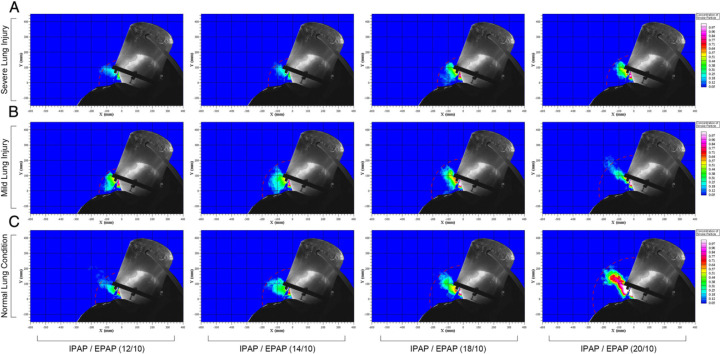
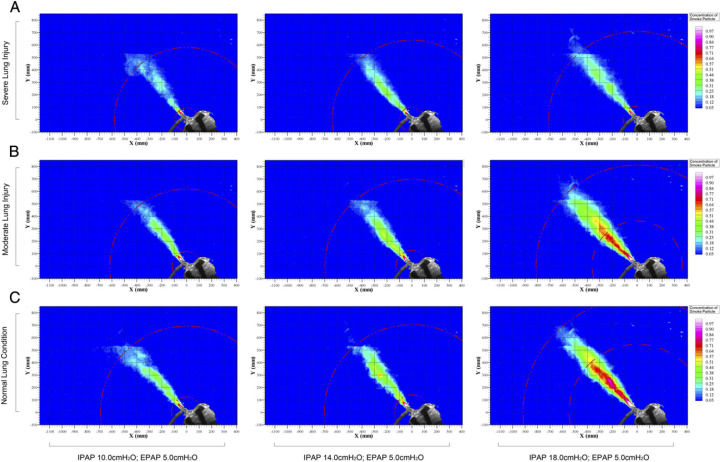
Results: During NIV via a helmet with the simulator programmed in mild lung injury, exhaled air leaked through the neck-helmet interface with a radial distance of 150 to 230 mm when inspiratory positive airway pressure was increased from 12 to 20 cm H2O, respectively, while keeping the expiratory pressure at 10 cm H2O. During NIV via a helmet with air cushion around the neck, there was negligible air leakage. During NIV via a total facemask for mild lung injury, air leaked through the exhalation port to 618 and 812 mm when inspiratory pressure was increased from 10 to 18 cm H2O, respectively, with the expiratory pressure at 5 cm H2O.
Conclusions: A helmet with a good seal around the neck is needed to prevent nosocomial infection during NIV for patients with respiratory infections.
Figures
Comment in
-
Navigating shifting waters: rapid response to change in the era of COVID-19.Intern Med J. 2020 Jul;50(7):786-790. doi: 10.1111/imj.14921. Intern Med J. 2020. PMID: 32656969 Free PMC article. No abstract available.
References
-
- Lee N, Hui D, Wu A. A major outbreak of severe acute respiratory syndrome in Hong Kong. N Engl J Med. 2003;348(20):1986–1994. - PubMed
-
- Abdel-Ghafar AN, Chotpitayasunondh T, Gao Z. Update on avian influenza A (H5N1) virus infection in humans. N Engl J Med. 2008;358(3):261–273. Writing Committee of the Second World Health Organization Consultation on Clinical Aspects of Human Infection with Avian Influenza A (H5N1) Virus. - PubMed
-
- Gao HN, Lu HZ, Cao B. Clinical findings in 111 cases of influenza A (H7N9) virus infection. N Engl J Med. 2013;368(24):2277–2285. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
