

Rational classification of portal vein thrombosis and its clinical significance
- PMID: 25393320
- PMCID: PMC4231054
- DOI: 10.1371/journal.pone.0112501
Rational classification of portal vein thrombosis and its clinical significance
Abstract
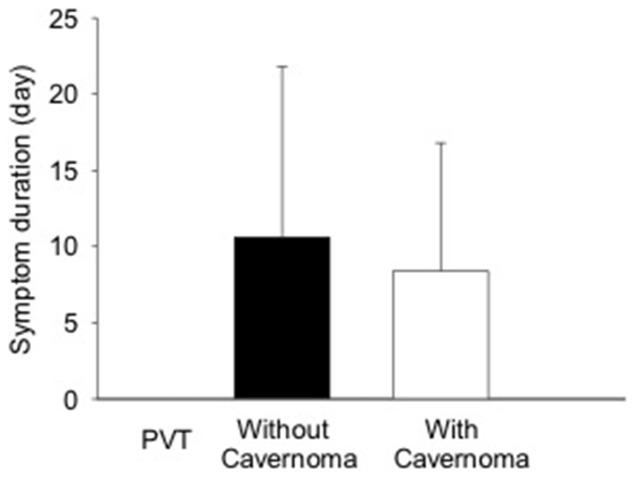
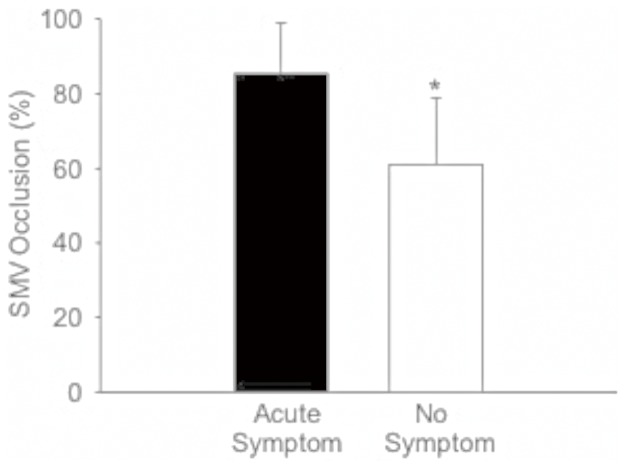
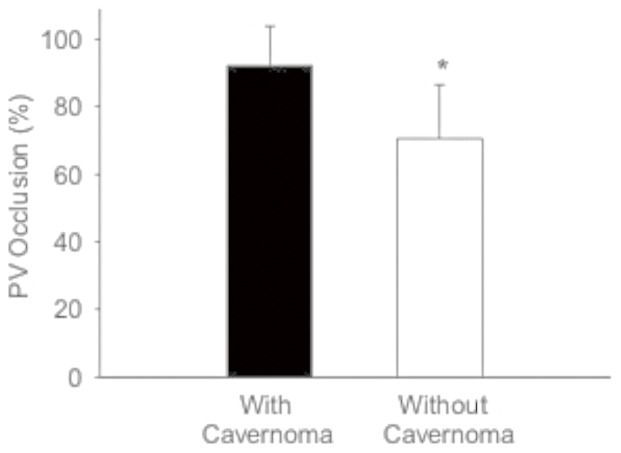
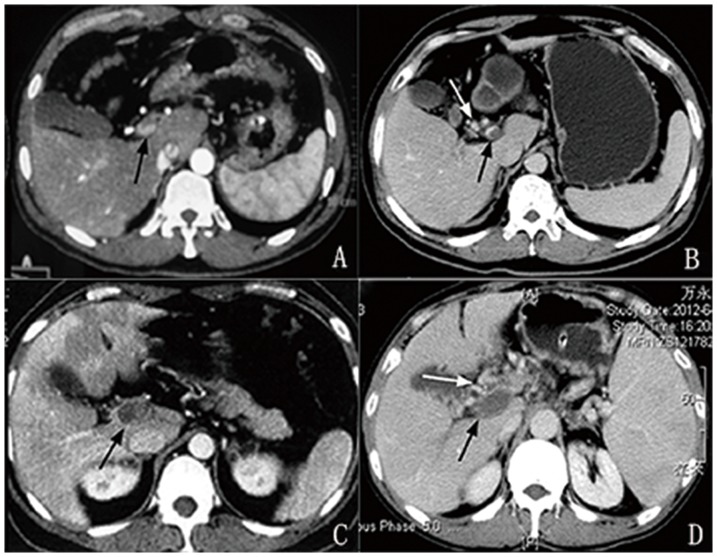
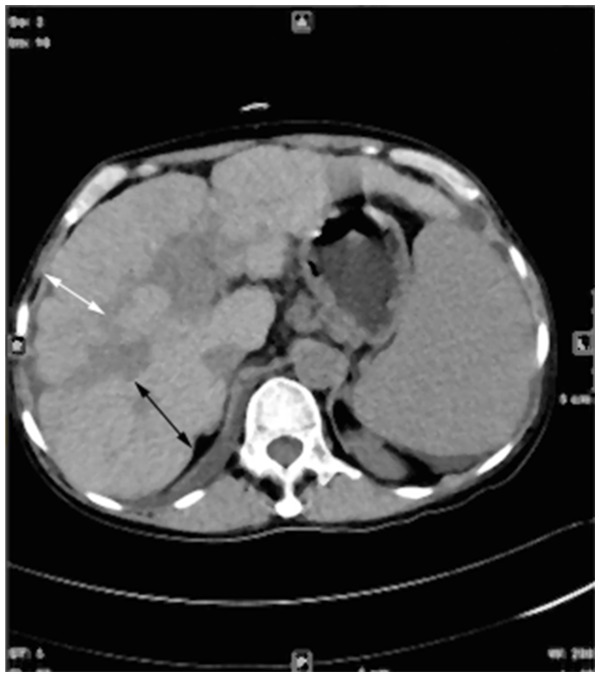
Portal vein thrombosis (PVT) is commonly classified into acute (symptom duration <60 days and absence of portal carvernoma and portal hypertension) and chronic types. However, the rationality of this classification has received little attention. In this study, 60 patients (40 men and 20 women) with PVT were examined using contrast-enhanced computed tomography (CT). The percentage of vein occlusion, including portal vein (PV) and superior mesenteric vein (SMV), was measured on CT image. Of 60 patients, 17 (28.3%) met the criterion of acute PVT. Symptoms occurred more frequently in patients with superior mesenteric vein thrombosis (SMVT) compared to those without SMVT (p<0.001). However, there was no significant difference in PV occlusion between patients with and without symptoms. The frequency of cavernous transformation was significantly higher in patients with complete PVT than those with partial PVT (p<0.001). Complications of portal hypertension were significantly associated with cirrhosis (p<0.001) rather than with the severity of PVT and presence of cavernoma. These results suggest that the severity of PVT is only associated with the formation of portal cavernoma but unrelated to the onset of symptoms and the development of portal hypertension. We classified PVT into complete and partial types, and each was subclassified into with and without portal cavernoma. In conclusion, neither symptom duration nor cavernous transformation can clearly distinguish between acute and chronic PVT. The new classification system can determine the pathological alterations of PVT, patency of portal vein and outcome of treatment in a longitudinal study.
Conflict of interest statement
Figures
References
-
- Hall TC, Garcea G, Metcalfe M, Bilku D, Dennison AR (2011) Management of acute non-cirrhotic and non-malignant portal vein thrombosis: a systematic review. World J Surg 35: 2510–2520. - PubMed
-
- James AW, Rabl C, Westphalen AC, Fogarty PF, Posselt AM, et al. (2009) Portomesenteric venous thrombosis after laparoscopic surgery: a systematic literature review. Arch Surg 144: 520–526. - PubMed
-
- Valla DC (2011) Portal vein thrombosis. In: Deleve LD, Garcia-Tsao G, editors. Vascular liver disease: Mechanisms and management. New York, Dordrecht Heidelberg, London: Springer Science+Bussiness Media, LLC. pp.183–196.
-
- Amitrano L, Guardascione MA, Scaglione M, Pezzullo L, Sangiuliano N, et al. (2007) Prognostic factors in noncirrhotic patients with splanchnic vein thromboses. Am J Gastroenterol 102: 2464–2470. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
