

Longitudinal analysis of T and B cell phenotype and function in renal transplant recipients with or without rituximab induction therapy
- PMID: 25393622
- PMCID: PMC4231065
- DOI: 10.1371/journal.pone.0112658
Longitudinal analysis of T and B cell phenotype and function in renal transplant recipients with or without rituximab induction therapy
Abstract
Background: Prevention of rejection after renal transplantation requires treatment with immunosuppressive drugs. Data on their in vivo effects on T- and B-cell phenotype and function are limited.
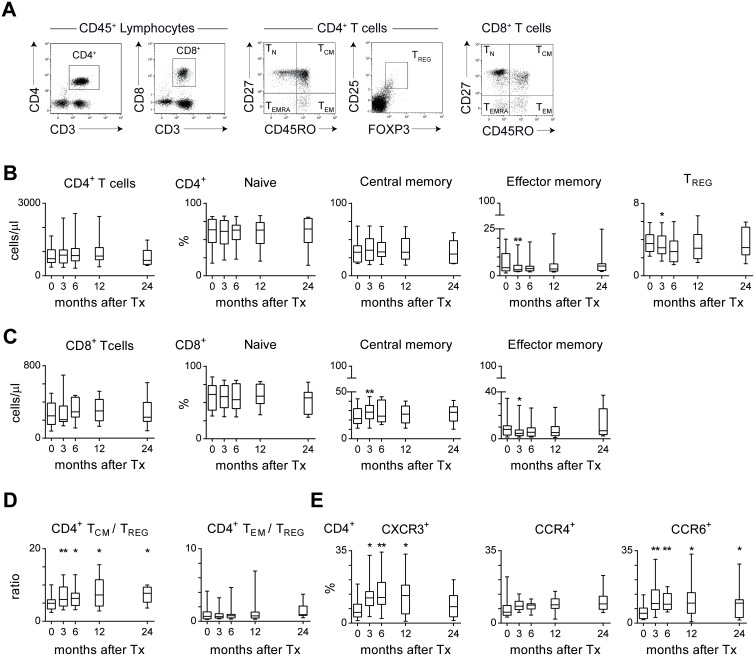
Methods: In a randomized double-blind placebo-controlled study to prevent renal allograft rejection, patients were treated with tacrolimus, mycophenolate mofetil (MMF), steroids, and a single dose of rituximab or placebo during transplant surgery. In a subset of patients, we analyzed the number and phenotype of peripheral T and B cells by multiparameter flow cytometry before transplantation, and at 3, 6, 12, and 24 months after transplantation.
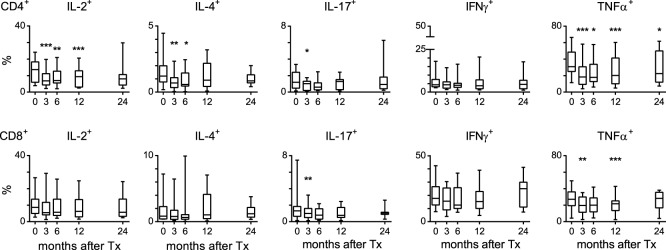
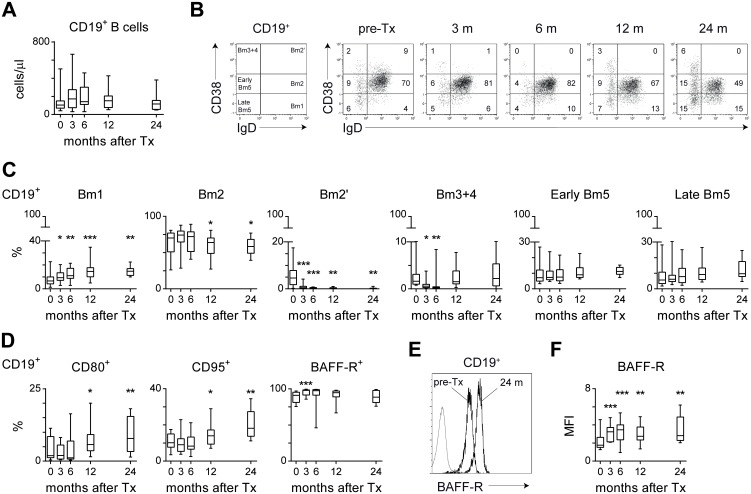
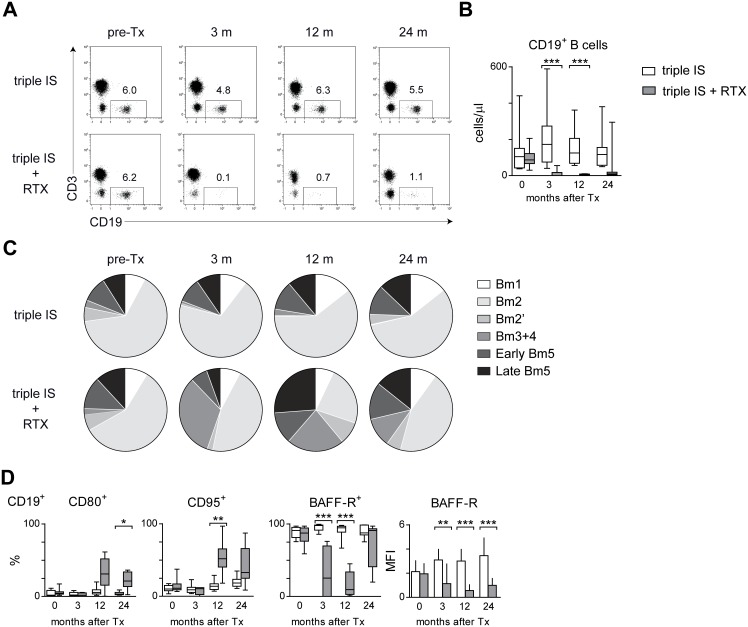
Results: In patients treated with tacrolimus/MMF/steroids the proportion of central memory CD4+ and CD8+ T cells was higher at 3 months post-transplant compared to pre-transplant levels. In addition, the ratio between the percentage of central memory CD4+ and CD4+ regulatory T cells was significantly higher up to 24 months post-transplant compared to pre-transplant levels. Interestingly, treatment with tacrolimus/MMF/steroids resulted in a shift toward a more memory-like B-cell phenotype post-transplant. Addition of a single dose of rituximab resulted in a long-lasting B-cell depletion. At 12 months post-transplant, the small fraction of repopulated B cells consisted of a high percentage of transitional B cells. Rituximab treatment had no effect on the T-cell phenotype and function post-transplant.
Conclusions: Renal transplant recipients treated with tacrolimus/MMF/steroids show an altered memory T and B-cell compartment post-transplant. Additional B-cell depletion by rituximab leads to a relative increase of transitional and memory-like B cells, without affecting T-cell phenotype and function.
Trial registration: ClinicalTrials.gov NCT00565331.
Conflict of interest statement
Figures
References
-
- Chapman JR, O’Connell PJ, Nankivell BJ (2005) Chronic renal allograft dysfunction. J Am Soc Nephrol 16: 3015–3026. - PubMed
-
- Safinia N, Afzali B, Atalar K, Lombardi G, Lechler RI (2010) T-cell alloimmunity and chronic allograft dysfunction. Kidney International 78 Suppl 119: S2–12. - PubMed
-
- Kahan BD (2003) Individuality: the barrier to optimal immunosuppression. Nat Rev Immunol 3: 831–838. - PubMed
-
- Wood KJ, Bushell A, Hester J (2012) Regulatory immune cells in transplantation. Nat Rev Immunol 12: 417–430. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
