

Thrombospondin type-1 domain-containing 7A in idiopathic membranous nephropathy
- PMID: 25394321
- PMCID: PMC4278759
- DOI: 10.1056/NEJMoa1409354
Thrombospondin type-1 domain-containing 7A in idiopathic membranous nephropathy
Abstract
Background: Idiopathic membranous nephropathy is an autoimmune disease. In approximately 70% of patients, it is associated with autoantibodies against the phospholipase A2 receptor 1 (PLA2R1). Antigenic targets in the remaining patients are unknown.
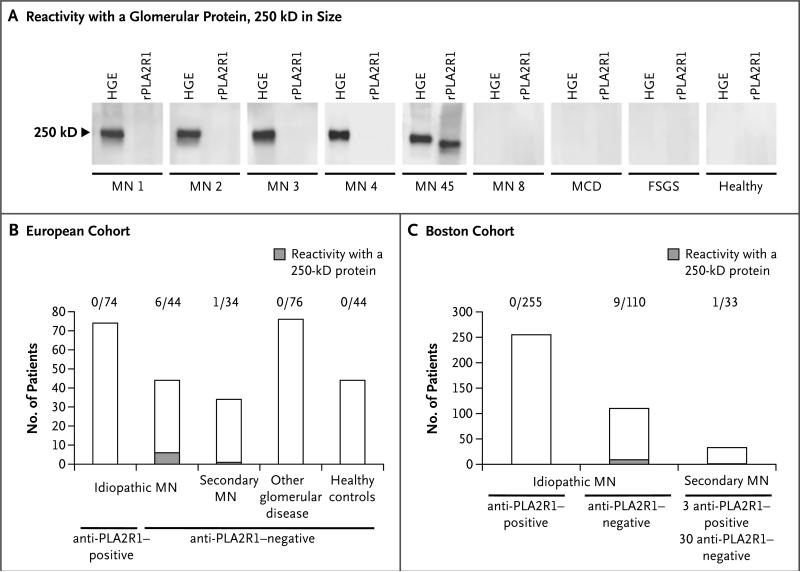
Methods: Using Western blotting, we screened serum samples from patients with idiopathic membranous nephropathy, patients with other glomerular diseases, and healthy controls for antibodies against human native glomerular proteins. We partially purified a putative new antigen, identified this protein by means of mass spectrometry of digested peptides, and validated the results by analysis of recombinant protein expression, immunoprecipitation, and immunohistochemical analysis.
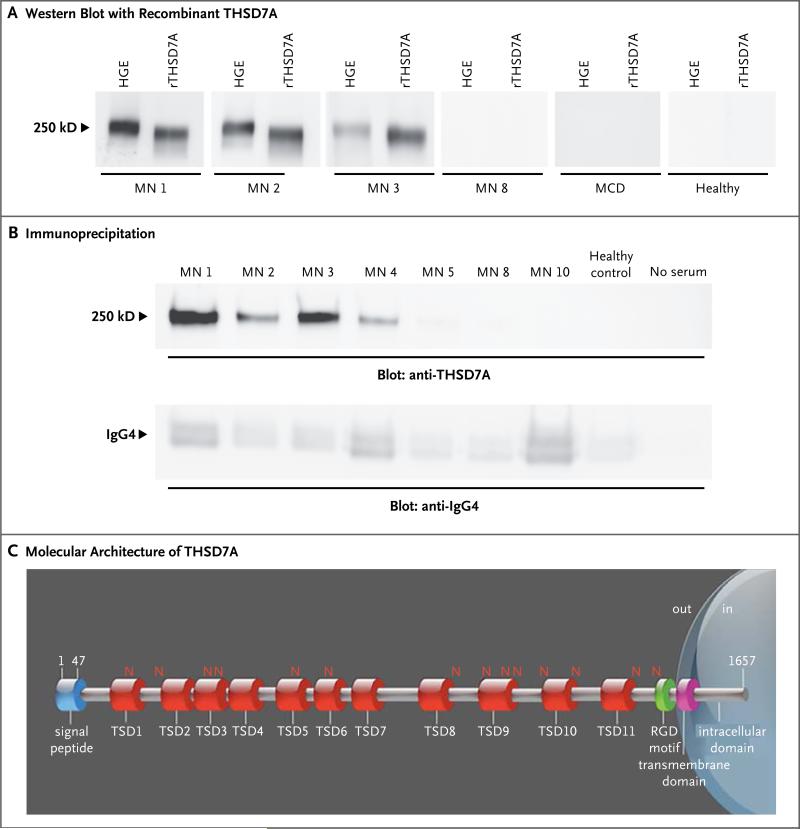
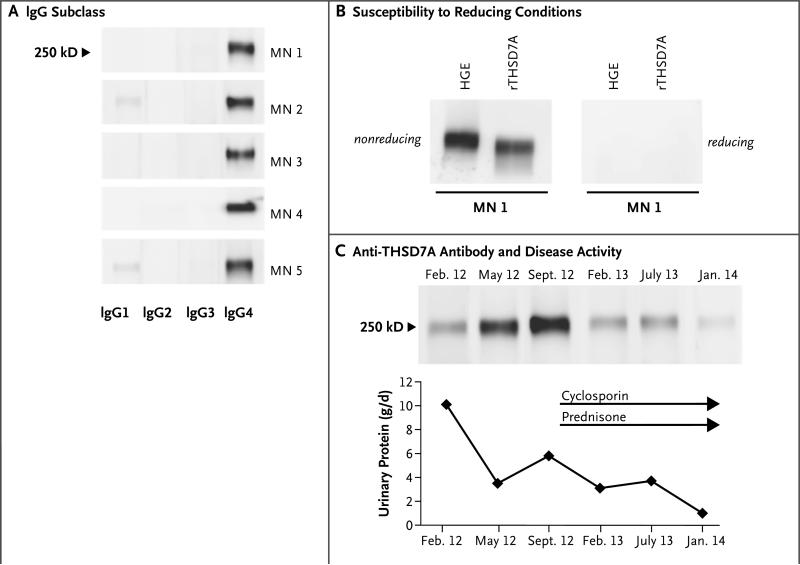
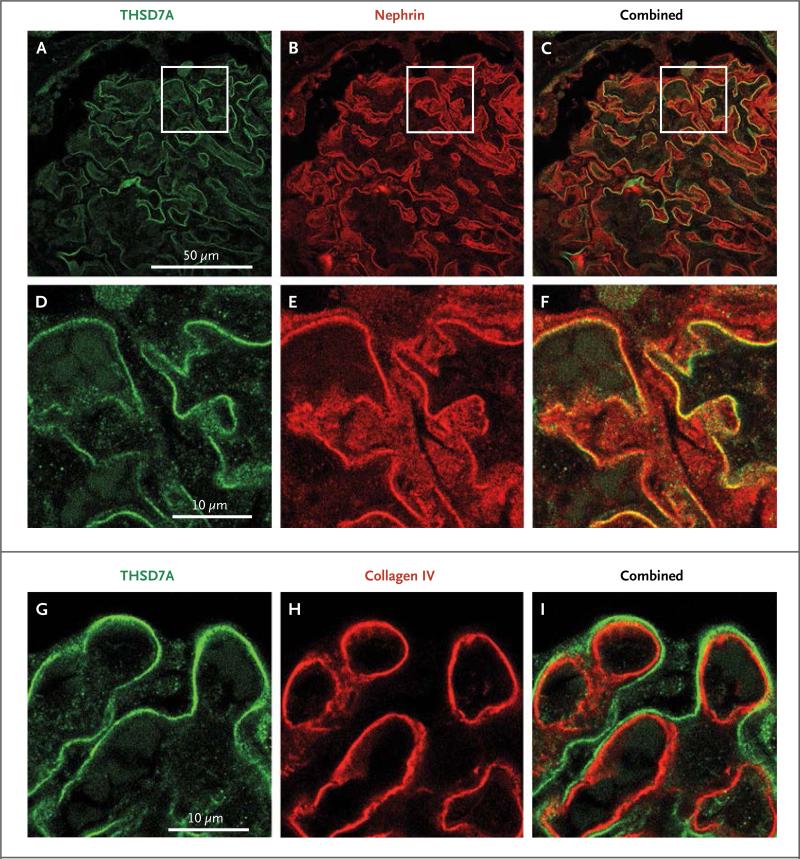
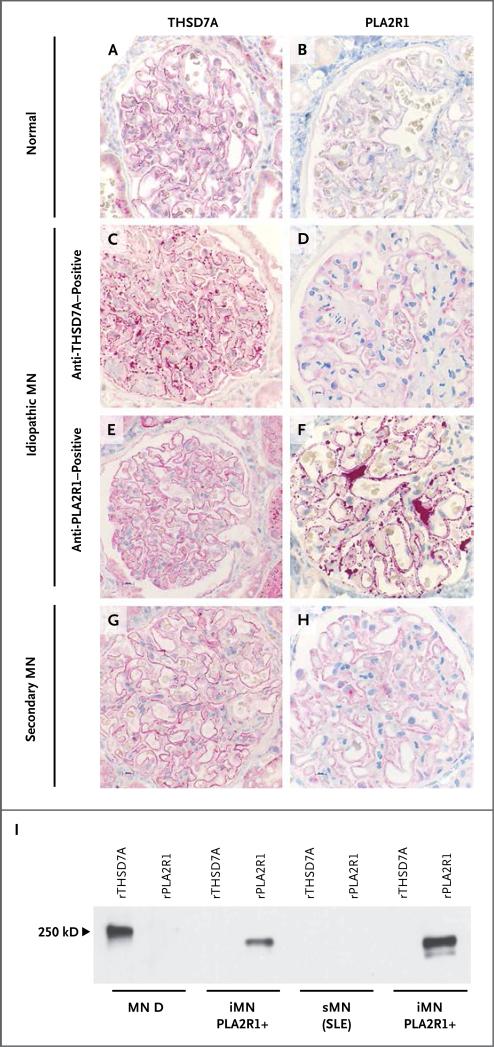
Results: Serum samples from 6 of 44 patients in a European cohort and 9 of 110 patients in a Boston cohort with anti-PLA2R1-negative idiopathic membranous nephropathy recognized a glomerular protein that was 250 kD in size. None of the serum samples from the 74 patients with idiopathic membranous nephropathy who were seropositive for anti-PLA2R1 antibodies, from the 76 patients with other glomerular diseases, and from the 44 healthy controls reacted against this antigen. Although this newly identified antigen is clearly different from PLA2R1, it shares some biochemical features, such as N-glycosylation, membranous location, and reactivity with serum only under nonreducing conditions. Mass spectrometry identified this antigen as thrombospondin type-1 domain-containing 7A (THSD7A). All reactive serum samples recognized recombinant THSD7A and immunoprecipitated THSD7A from glomerular lysates. Moreover, immunohistochemical analyses of biopsy samples from patients revealed localization of THSD7A to podocytes, and IgG eluted from one of these samples was specific for THSD7A.
Conclusions: In our cohort, 15 of 154 patients with idiopathic membranous nephropathy had circulating autoantibodies to THSD7A but not to PLA2R1, a finding that suggests a distinct subgroup of patients with this condition. (Funded by the French National Center for Scientific Research and others.).
Figures
Comment in
-
Glomerular disease: thrombospondin type-1 domain-containing 7A-a new player in membranous nephropathy.Nat Rev Nephrol. 2015 Feb;11(2):63. doi: 10.1038/nrneph.2014.227. Epub 2014 Dec 2. Nat Rev Nephrol. 2015. PMID: 25447129 No abstract available.
-
Thrombospondin type-1 domain-containing 7A in idiopathic membranous nephropathy.N Engl J Med. 2015 Mar 12;372(11):1074-5. doi: 10.1056/NEJMc1500130. N Engl J Med. 2015. PMID: 25760364 No abstract available.
-
Thrombospondin type-1 domain-containing 7A in idiopathic membranous nephropathy.N Engl J Med. 2015 Mar 12;372(11):1073. doi: 10.1056/NEJMc1500130. N Engl J Med. 2015. PMID: 25760365 No abstract available.
References
-
- Deegens JK, Wetzels JF. Membranous nephropathy in the older adult: epidemiology, diagnosis and management. Drugs Aging. 2007;24:717–32. - PubMed
-
- Hoxha E, Harendza S, Zahner G, et al. An immunofluorescence test for phospholipase-A₂-receptor antibodies and its clinical usefulness in patients with mem branous glomerulonephritis. Nephrol Dial Transplant. 2011;26:2526–32. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases