

Sepsis-associated hyperlactatemia
- PMID: 25394679
- PMCID: PMC4421917
- DOI: 10.1186/s13054-014-0503-3
Sepsis-associated hyperlactatemia
Abstract
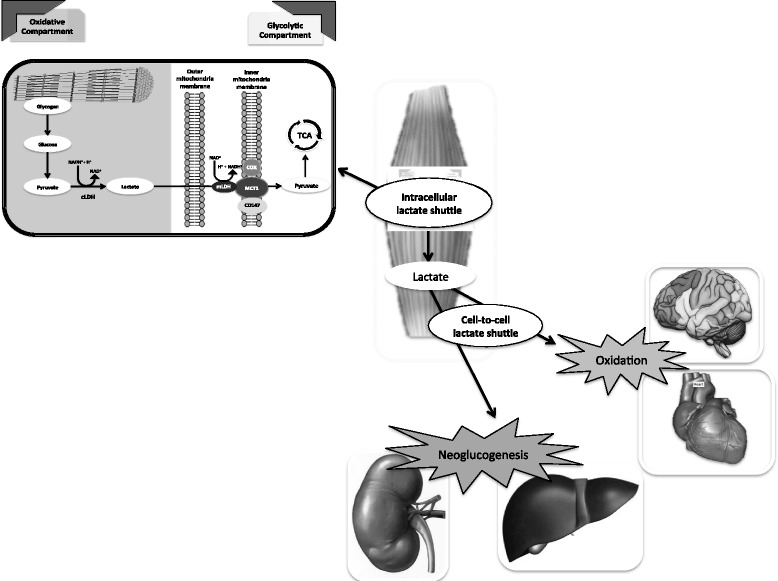
There is overwhelming evidence that sepsis and septic shock are associated with hyperlactatemia (sepsis-associated hyperlactatemia (SAHL)). SAHL is a strong independent predictor of mortality and its presence and progression are widely appreciated by clinicians to define a very high-risk population. Until recently, the dominant paradigm has been that SAHL is a marker of tissue hypoxia. Accordingly, SAHL has been interpreted to indicate the presence of an 'oxygen debt' or 'hypoperfusion', which leads to increased lactate generation via anaerobic glycolysis. In light of such interpretation of the meaning of SAHL, maneuvers to increase oxygen delivery have been proposed as its treatment. Moreover, lactate levels have been proposed as a method to evaluate the adequacy of resuscitation and the nature of the response to the initial treatment for sepsis. However, a large body of evidence has accumulated that strongly challenges such notions. Much evidence now supports the view that SAHL is not due only to tissue hypoxia or anaerobic glycolysis. Experimental and human studies all consistently support the view that SAHL is more logically explained by increased aerobic glycolysis secondary to activation of the stress response (adrenergic stimulation). More importantly, new evidence suggests that SAHL may actually serve to facilitate bioenergetic efficiency through an increase in lactate oxidation. In this sense, the characteristics of lactate production best fit the notion of an adaptive survival response that grows in intensity as disease severity increases. Clinicians need to be aware of these developments in our understanding of SAHL in order to approach patient management according to biological principles and to interpret lactate concentrations during sepsis resuscitation according to current best knowledge.
Figures


References
-
- Jansen TC, van Bommel J, Schoonderbeek FJ, Sleeswijk Visser SJ, van der Klooster JM, Lima AP, Willemsen SP, Bakker J. Early lactate-guided therapy in intensive care unit patients: a multicenter, open-label, randomized controlled trial. Am J Respir Crit Care Med. 2010;182:752–761. doi: 10.1164/rccm.200912-1918OC. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
