

Universes collide: combining immunotherapy with targeted therapy for cancer
- PMID: 25395294
- PMCID: PMC4258160
- DOI: 10.1158/2159-8290.CD-14-0477
Universes collide: combining immunotherapy with targeted therapy for cancer
Abstract
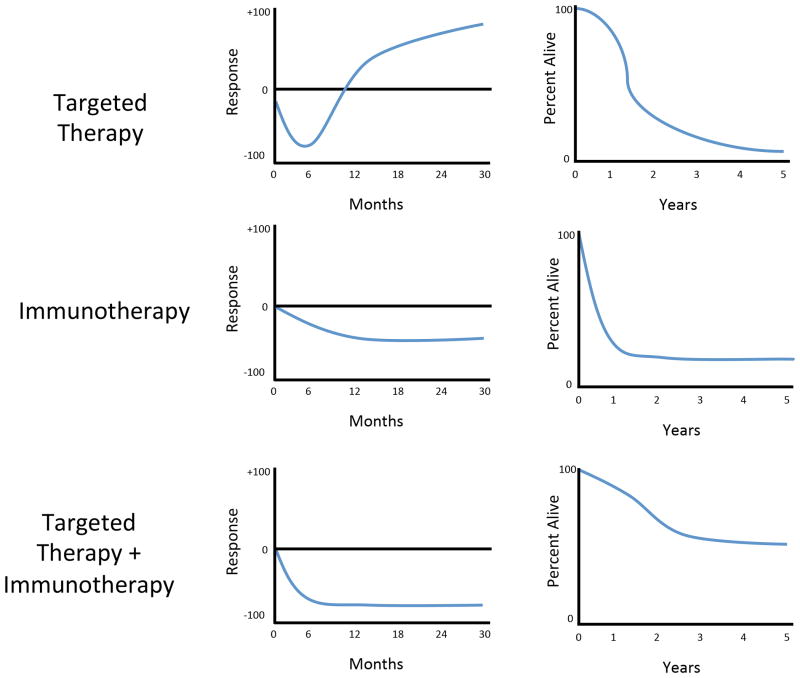
There have been significant advances in the past several years with regard to targeted therapy and immunotherapy for cancer. This is highlighted in melanoma, where treatment with targeted therapy (against the BRAF oncoprotein) results in responses in the majority of patients, although the duration of response is limited. In contrast, treatment with immunotherapy results in a lower response rate, but one that tends to be more durable. Insights about mechanisms of response and potential synergy between these treatment strategies for melanoma are a focus of this review, with opportunities to extend these insights to the treatment of other cancers.
Significance: Two major advances in melanoma have occurred concurrently and involve treatment with targeted therapy and immune checkpoint blockade. However, each of these approaches has limitations with regard to overall response rates or duration of response. To address this, investigators have proposed combining these strategies, and this concept is being tested empirically in clinical trials. There is a scientific rationale supporting the combination of targeted therapy and immunotherapy, and these concepts are discussed herein.
©2014 American Association for Cancer Research.
Conflict of interest statement
Figures
References
-
- Davies H, Bignell GR, Cox C, Stephens P, Edkins S, Clegg S, et al. Mutations of the BRAF gene in human cancer. Nature. 2002;417:949–54. - PubMed
-
- Hauschild A, Grob JJ, Demidov LV, Jouary T, Gutzmer R, Millward M, et al. Dabrafenib in BRAF-mutated metastatic melanoma: a multicentre, open-label, phase 3 randomised controlled trial. Lancet. 2012;380:358–65. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
Miscellaneous
