

Conscious sedation versus general anesthesia during endovascular acute ischemic stroke treatment: a systematic review and meta-analysis
- PMID: 25395655
- PMCID: PMC8013063
- DOI: 10.3174/ajnr.A4159
Conscious sedation versus general anesthesia during endovascular acute ischemic stroke treatment: a systematic review and meta-analysis
Abstract
Background and purpose: A number of studies have suggested that anesthesia type (conscious sedation versus general anesthesia) during intra-arterial treatment for acute ischemic stroke has implications for patient outcomes. We performed a systematic review and meta-analysis of studies comparing the clinical and angiographic outcomes of the 2 anesthesia types.
Materials and methods: In March 2014, we conducted a computerized search of MEDLINE and EMBASE for reports on anesthesia and endovascular treatment of acute ischemic stroke. Using random-effects meta-analysis, we evaluated the following outcomes: recanalization rate, good functional outcome (mRS ≤ 2), asymptomatic and symptomatic intracranial hemorrhage, death, vascular complications, respiratory complications, procedure time, time to groin, and time from symptom onset to recanalization.
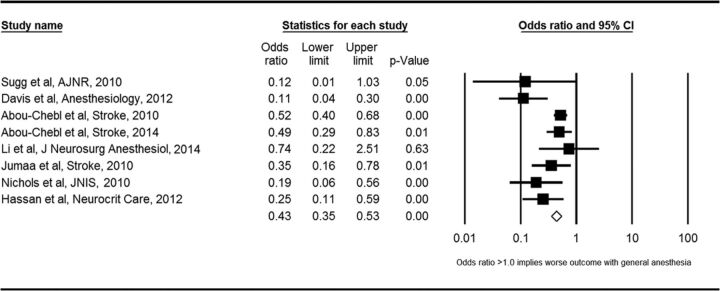
Results: Nine studies enrolling 1956 patients (814 with general anesthesia and 1142 with conscious sedation) were included. Compared with patients treated by using conscious sedation during stroke intervention, patients undergoing general anesthesia had higher odds of death (OR = 2.59; 95% CI, 1.87-3.58) and respiratory complications (OR = 2.09; 95% CI, 1.36-3.23) and lower odds of good functional outcome (OR = 0.43; 95% CI, 0.35-0.53) and successful angiographic outcome (OR = 0.54; 95% CI, 0.37-0.80). No difference in procedure time (P = .28) was seen between the groups. Preintervention NIHSS scores were available from 6 studies; in those, patients receiving general anesthesia had a higher average NIHSS score.
Conclusions: Patients with acute ischemic stroke undergoing intra-arterial therapy may have worse outcomes with general anesthesia compared with conscious sedation. However, the difference in stroke severity at the onset may confound the comparison in the available studies; thus, a randomized trial is necessary to confirm this association.
© 2015 by American Journal of Neuroradiology.
Figures
References
-
- Brinjikji W, Rabinstein AA, Kallmes DF, et al. . Patient outcomes with endovascular embolectomy therapy for acute ischemic stroke: a study of the National Inpatient Sample: 2006 to 2008. Stroke 2011;42:1648–52 - PubMed
-
- Saver JL. Time is brain–quantified. Stroke 2006;37:263–66 - PubMed
-
- Molina CA, Selim MH. General or local anesthesia during endovascular procedures: sailing quiet in the darkness or fast under a daylight storm. Stroke 2010;41:2720–21 - PubMed
-
- Brekenfeld C, Mattle HP, Schroth G. General is better than local anesthesia during endovascular procedures. Stroke 2010;41:2716–17 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical