

Peripheral response to cervical or thoracic spinal manual therapy: an evidence-based review with meta analysis
- PMID: 25395830
- PMCID: PMC4215103
- DOI: 10.1179/2042618613Y.0000000062
Peripheral response to cervical or thoracic spinal manual therapy: an evidence-based review with meta analysis
Abstract
Objectives: Spinal manual therapy (SMT) is commonly used for treatment of musculoskeletal pain in the neck, upper back, or upper extremity. Some authors report a multi-system effect of SMT, including peripheral alterations in skin conductance and skin temperature, suggesting that SMT may initiate a sympathetic nervous system (SNS) response. The focus of this evidence-based review and meta-analysis is to evaluate the evidence of SNS responses and clinically relevant outcomes following SMT to the cervical or thoracic spine.
Methods: A SYSTEMATIC SEARCH USED THE TERMS: 'manual therapy', 'SMT', 'spinal manipulation', 'mobilization', 'SNS', 'autonomic nervous system', 'neurophysiology', 'hypoalgesia', 'pain pathophysiology', 'cervical vertebrae', 'thoracic vertebrae', 'upper extremity', and 'neurodynamic test'. Data were extracted and within-group and between-group effect sizes were calculated for outcomes of skin conductance, skin temperature, pain, and upper extremity range of motion (ROM) during upper limb neurodynamic tests (ULNTs).
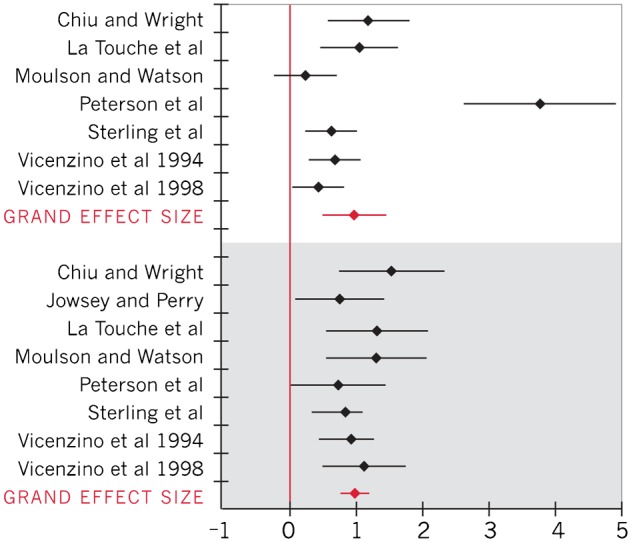
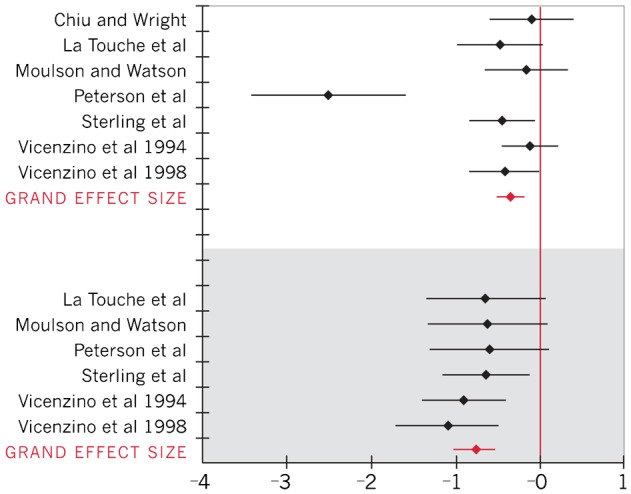
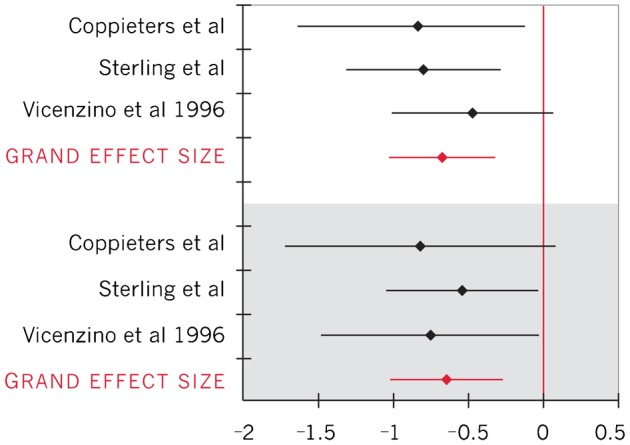
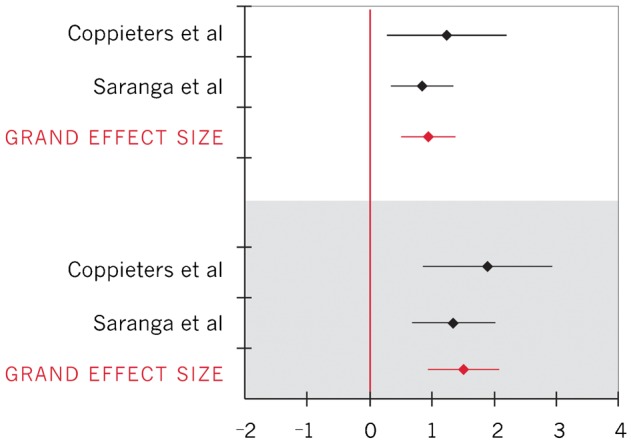
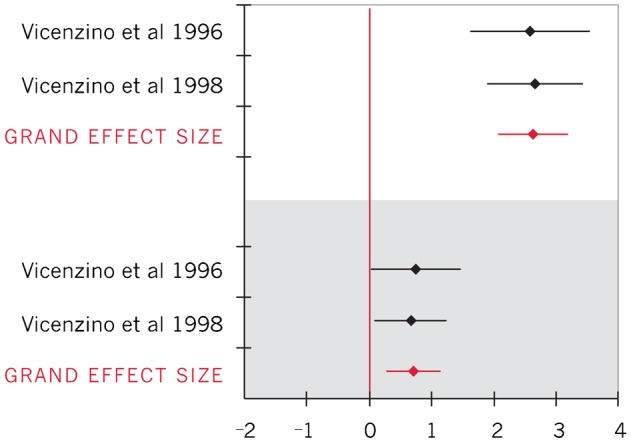
Results: Eleven studies were identified. Statistically significant changes were seen with increased skin conductance, decreased skin temperature, decreased pain, and increased upper extremity ROM during ULNT.
Discussion: A mechanical stimulus at the cervical or thoracic spine can produce a SNS excitatory response (increased skin conductance and decreased skin temperature). Findings of reduced pain and increased ROM during ULNT provide support to the clinical relevance of SMT. This evidence points toward additional mechanisms underlying the therapeutic effect of SMT. The effect sizes are small to moderate and no long-term effects post-SMT were collected. Future research is needed to associate peripheral effects with a possible centrally-mediated response to SMT.
Keywords: Cervical spine; Spinal manual therapy; Sympathetic nervous system; Thoracic spine.
Figures
References
-
- United States Bone and Joint Initiative. The Burden of Musculoskeletal Diseases in the United States, Second Edition. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2011.
-
- Evans D. Mechanisms and effects of spinal high-velocity low-amplitude thrust manipulation: previous theories. J Manipulative Physiol Ther. 2002;25:251–62. - PubMed
-
- Maigne JY, Vautravers P. Mechanism of action of spinal manipulative therapy. Joint Bone Spine. 2003;70:336–41. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical