

Potential drug-drug interactions in hospitalized patients with chronic heart failure and chronic obstructive pulmonary disease
- PMID: 25395943
- PMCID: PMC4223137
- DOI: 10.5114/aoms.2014.46212
Potential drug-drug interactions in hospitalized patients with chronic heart failure and chronic obstructive pulmonary disease
Abstract
Introduction: Polypharmacy is common in patients with chronic heart failure (HF) and/or chronic obstructive pulmonary disease (COPD), but little is known about the prevalence and significance of drug-drug interactions (DDIs). This study evaluates DDIs in hospitalized patients.
Material and methods: We retrospectively screened medical charts over a 6-month period for diagnosis of chronic HF and/or COPD. Potential DDIs were evaluated using Lexi-Interact software.
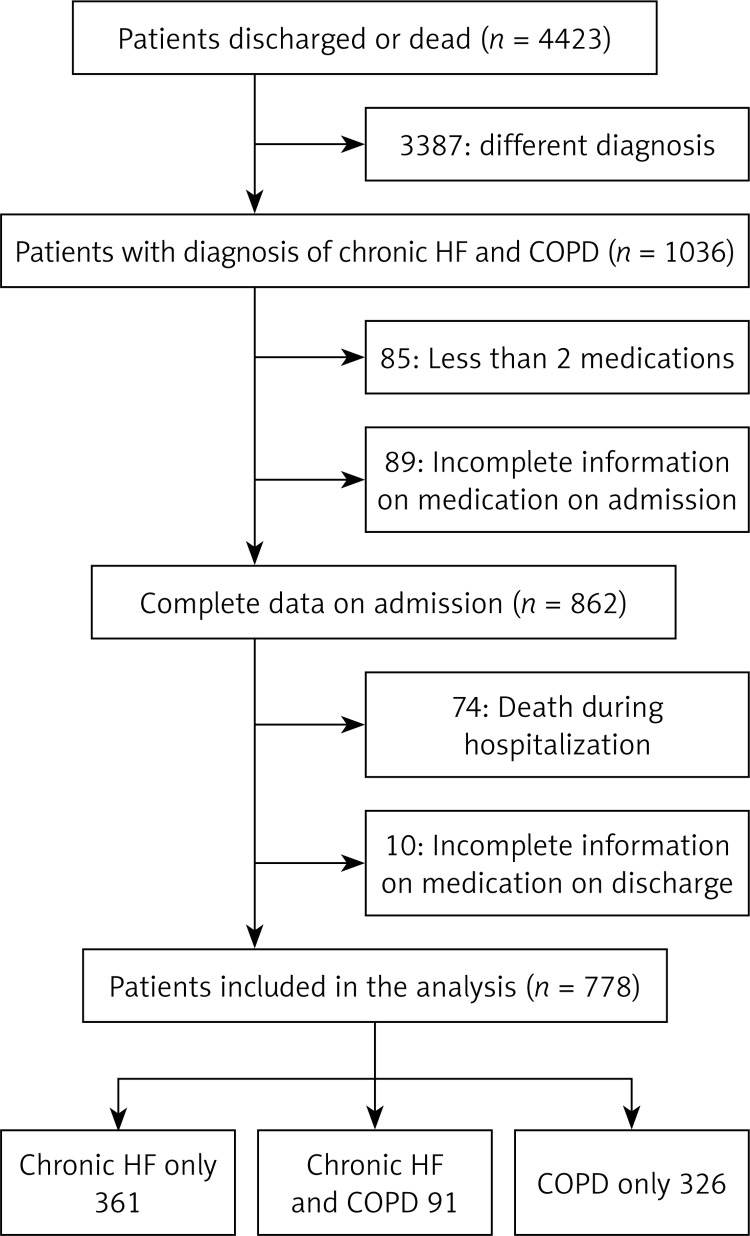
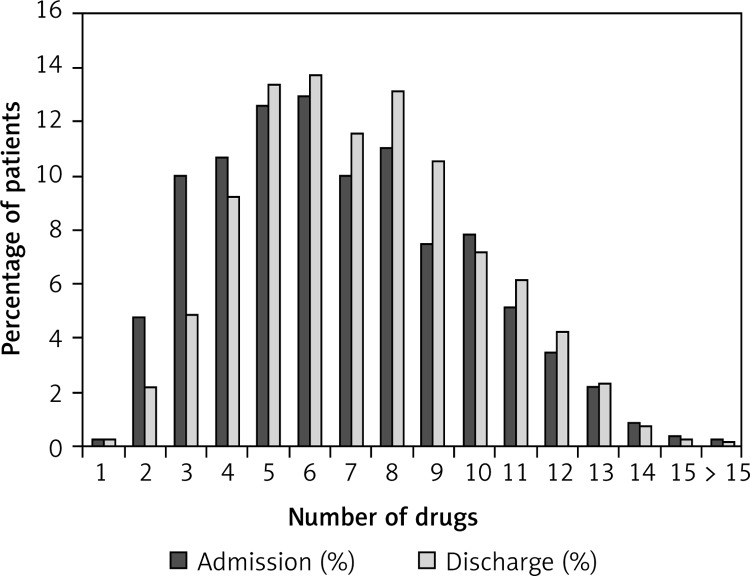
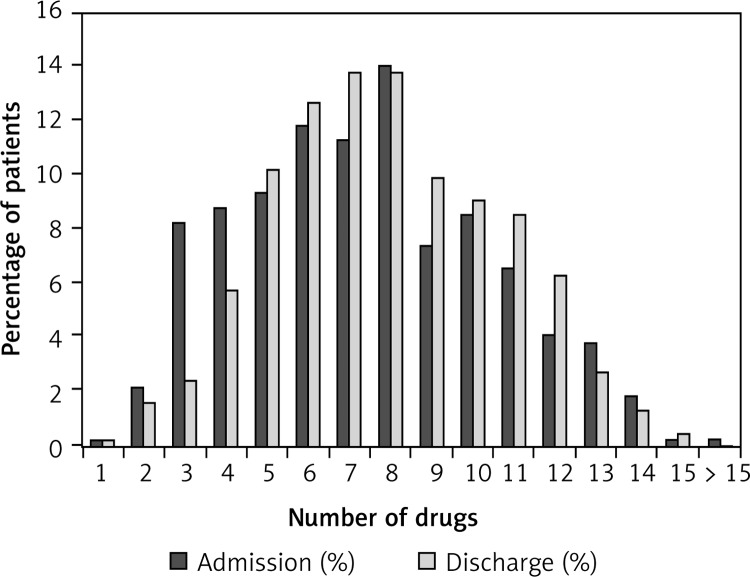
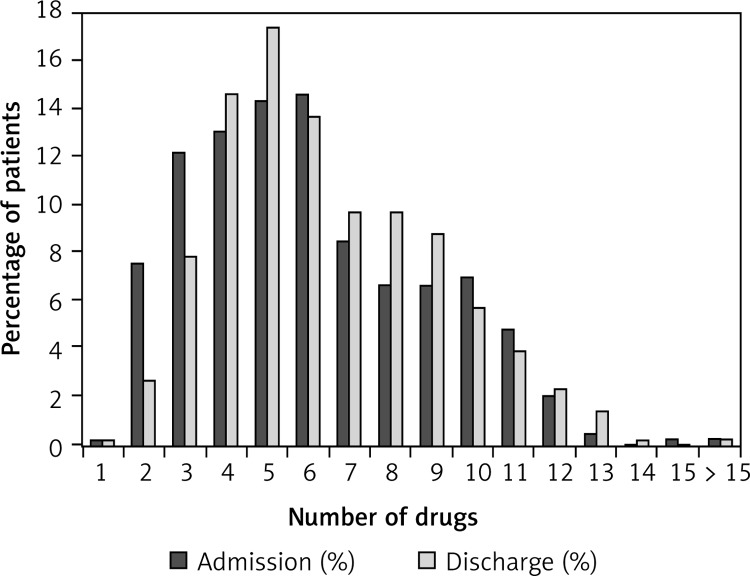
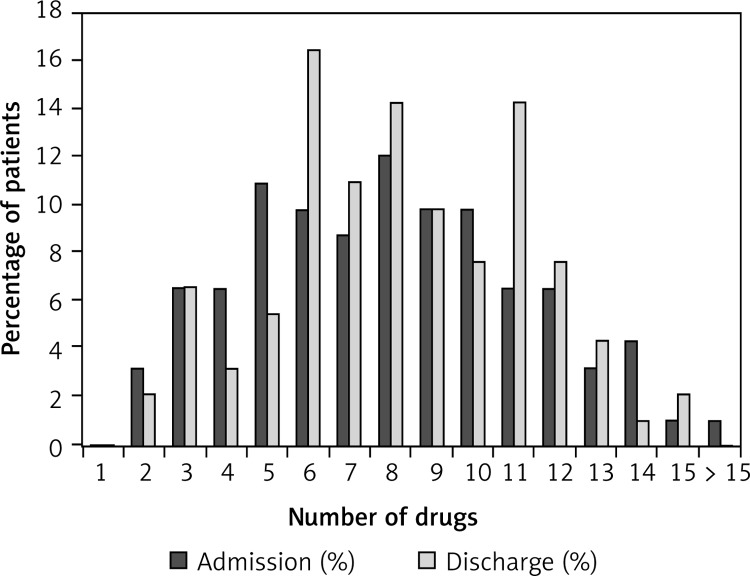
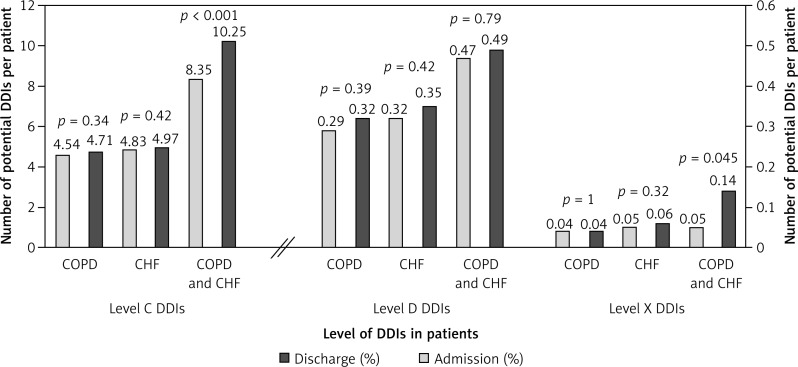
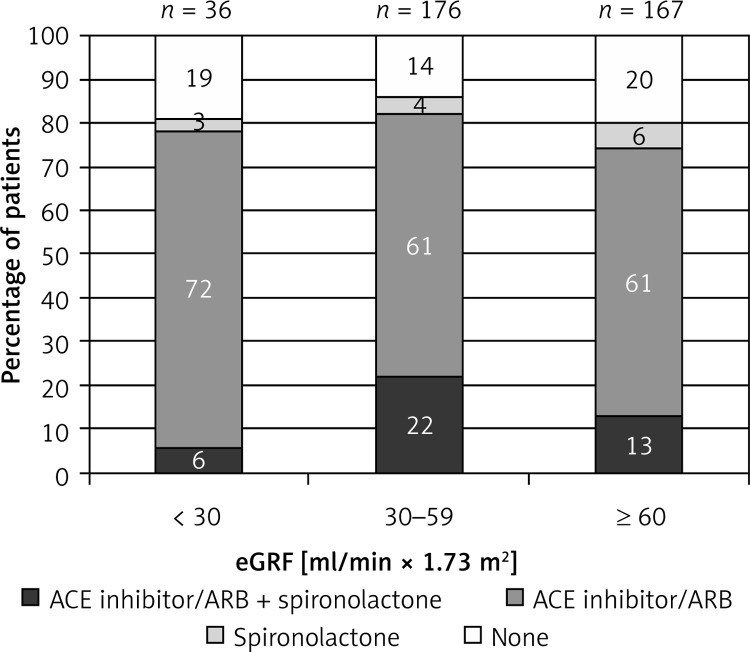
Results: Seven hundred and seventy-eight patients were included in the study (median age 75 years, 61% men). The median number of drugs on admission and discharge was 6 (interquartile range (IQR) 4-9) and 7 (IQR 5-), respectively (p = 0.10). We recorded 6.5 ±5.7 potential DDIs per patient on admission and 7.2 ±5.6 on discharge (p = 0.2). From admission to discharge, type-C and type-X potential DDIs increased (p < 0.05 for both). Type X interactions were rare (< 1%), with the combination of a β-blocker and a β2 agonist being the most common (64%). There were significantly more type-C and type-D potential DDIs in patients with chronic HF as compared to patients with COPD (p < 0.001). Patients with concomitant chronic HF and COPD had more type-C and type-X potential DDIs when compared to those with individual disease (p < 0.005). An aldosterone antagonist and ACE inhibitor/ARB were prescribed to 3% of chronic HF patients with estimated glomerular filtration rate < 30 ml/(min × 1.73 m(2)).
Conclusions: The DDIs are common in patients with chronic HF and/or COPD, but only a few appear to be of clinical significance. The increase in potential DDIs from admission to discharge may reflect better guideline implementation rather than poor clinical practice.
Keywords: chronic heart failure; chronic obstructive pulmonary disease; potential drug-drug interactions.
Figures
References
-
- Moura C, Acurcio F, Belo N. Drug-drug interactions associated with length of stay and cost of hospitalization. J Pharm Pharmaceut Sci. 2009;12:266–72. - PubMed
-
- Juurlink DM, Mamdani M, Kopp A, et al. Drug-drug interactions among elderly patients hospitalized for drug toxicity. JAMA. 2003;289:1652–8. - PubMed
-
- Björkman KI, Fastborn J, Schmidt IK, et al. Drug-drug interactions in elderly. Ann Pharmacother. 2002;36:1675–81. - PubMed
-
- Gallagher P, Barry P, O'Mahony D. Inappropriate prescribing in the elderly. J Clin Pharm Ther. 2007;32:113–21. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous