

Effects of increased von Willebrand factor levels on primary hemostasis in thrombocytopenic patients with liver cirrhosis
- PMID: 25397410
- PMCID: PMC4232392
- DOI: 10.1371/journal.pone.0112583
Effects of increased von Willebrand factor levels on primary hemostasis in thrombocytopenic patients with liver cirrhosis
Abstract
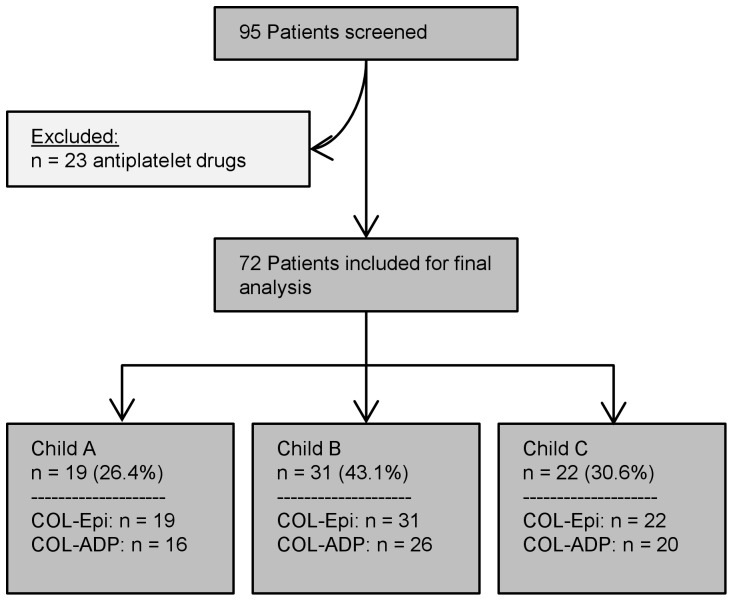
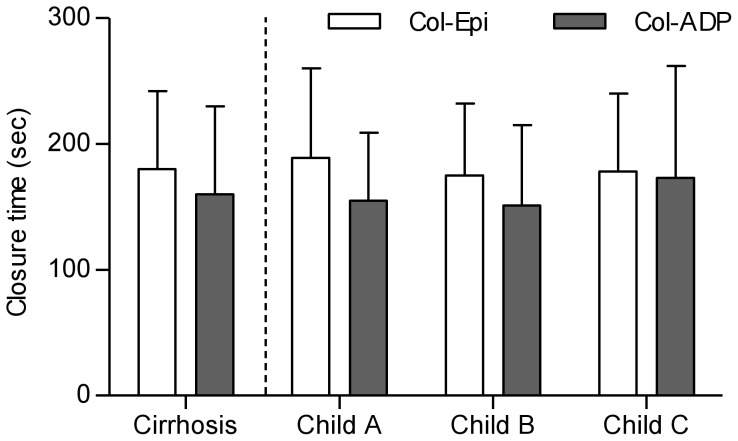
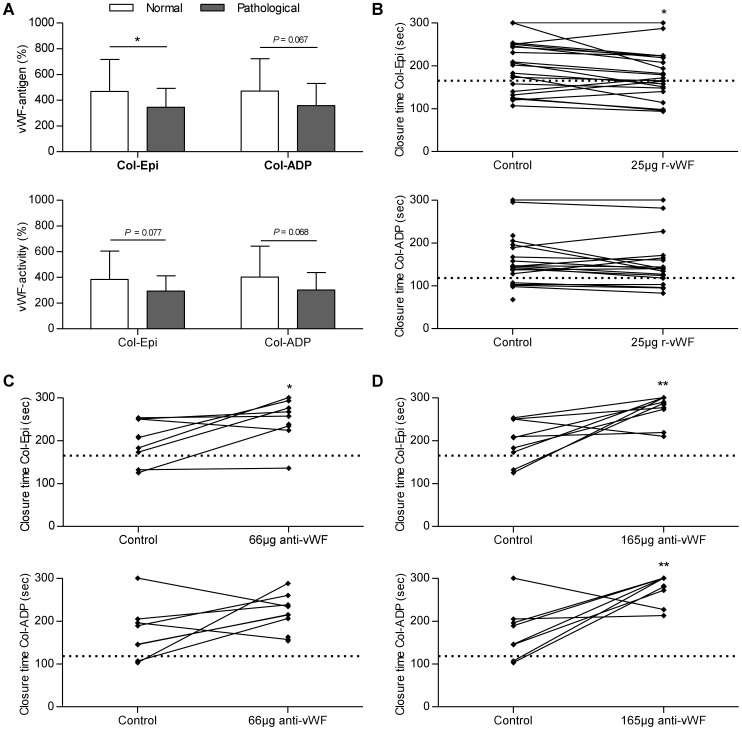
In patients with liver cirrhosis procoagulant and anticoagulant changes occur simultaneously. During primary hemostasis, platelets adhere to subendothelial structures, via von Willebrand factor (vWF). We aimed to investigate the influence of vWF on primary hemostasis in patients with liver cirrhosis. Therefore we assessed in-vitro bleeding time as marker of primary hemostasis in cirrhotic patients, measuring the Platelet Function Analyzer (PFA-100) closure times with collagen and epinephrine (Col-Epi, upper limit of normal ≤ 165 s) or collagen and ADP (Col-ADP, upper limit of normal ≤ 118 s). If Col-Epi and Col-ADP were prolonged, the PFA-100 was considered to be pathological. Effects of vWF on primary hemostasis in thrombocytopenic patients were analyzed and plasma vWF levels were modified by adding recombinant vWF or anti-vWF antibody. Of the 72 included cirrhotic patients, 32 (44.4%) showed a pathological result for the PFA-100. They had mean closure times (± SD) of 180 ± 62 s with Col-Epi and 160 ± 70 s with Col-ADP. Multivariate analysis revealed that hematocrit (P = 0.027) and vWF-antigen levels (P = 0.010) are the predictors of a pathological PFA-100 test in cirrhotic patients. In 21.4% of cirrhotic patients with platelet count ≥ 150/nL and hematocrit ≥ 27.0%, pathological PFA-100 results were found. In thrombocytopenic (< 150/nL) patients with cirrhosis, normal PFA-100 results were associated with higher vWF-antigen levels (462.3 ± 235.9% vs. 338.7 ± 151.6%, P = 0.021). These results were confirmed by multivariate analysis in these patients as well as by adding recombinant vWF or polyclonal anti-vWF antibody that significantly shortened or prolonged closure times, respectively. In conclusion, primary hemostasis is impaired in cirrhotic patients. The effect of reduced platelet count in cirrhotic patients can at least be partly compensated by increased vWF levels. Recombinant vWF could be an alternative to platelet transfusions in the future.
Conflict of interest statement
Figures
References
-
- Tripodi A, Mannucci PM (2011) The coagulopathy of chronic liver disease. N Engl J Med 365: 147–156. - PubMed
-
- Lisman T, Porte RJ (2010) The role of platelets in liver inflammation and regeneration. Semin Thromb Hemost 36: 170–174. - PubMed
-
- Sogaard KK, Horvath-Puho E, Gronbaek H, Jepsen P, Vilstrup H, et al. (2009) Risk of venous thromboembolism in patients with liver disease: a nationwide population-based case-control study. Am J Gastroenterol 104: 96–101. - PubMed
-
- Amitrano L, Guardascione MA, Brancaccio V, Margaglione M, Manguso F, et al. (2004) Risk factors and clinical presentation of portal vein thrombosis in patients with liver cirrhosis. J Hepatol 40: 736–741. - PubMed
-
- Sakariassen KS, Bolhuis PA, Sixma JJ (1979) Human blood platelet adhesion to artery subendothelium is mediated by factor VIII-Von Willebrand factor bound to the subendothelium. Nature 279: 636–638. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
