

Is early oral feeding after gastric cancer surgery feasible? A systematic review and meta-analysis of randomized controlled trials
- PMID: 25397686
- PMCID: PMC4232373
- DOI: 10.1371/journal.pone.0112062
Is early oral feeding after gastric cancer surgery feasible? A systematic review and meta-analysis of randomized controlled trials
Abstract
Aim: To assess the feasibility and safety of early oral feeding (EOF) after gastrectomy for gastric cancer through a systematic review and meta-analysis based on randomized controlled trials.
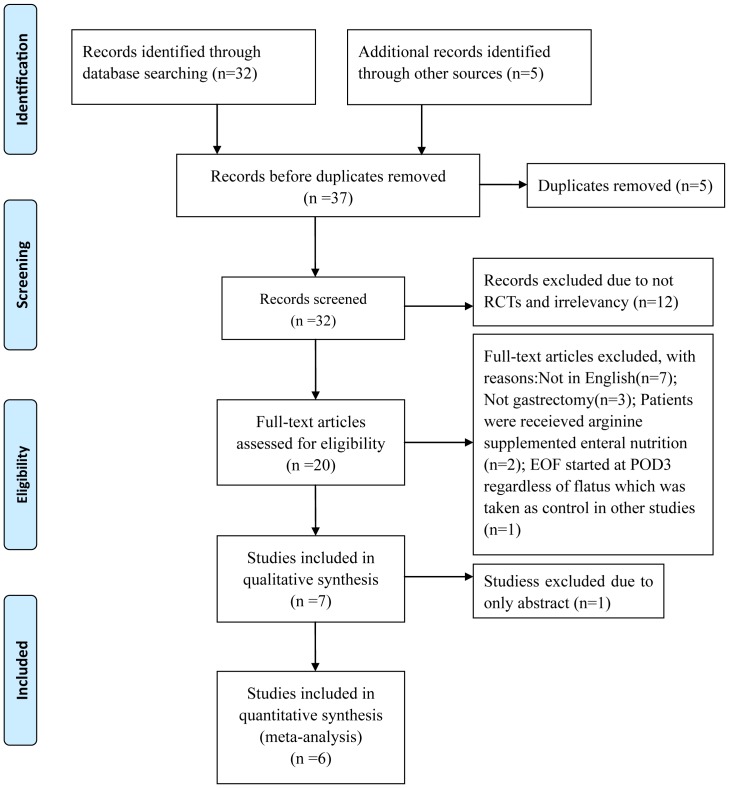
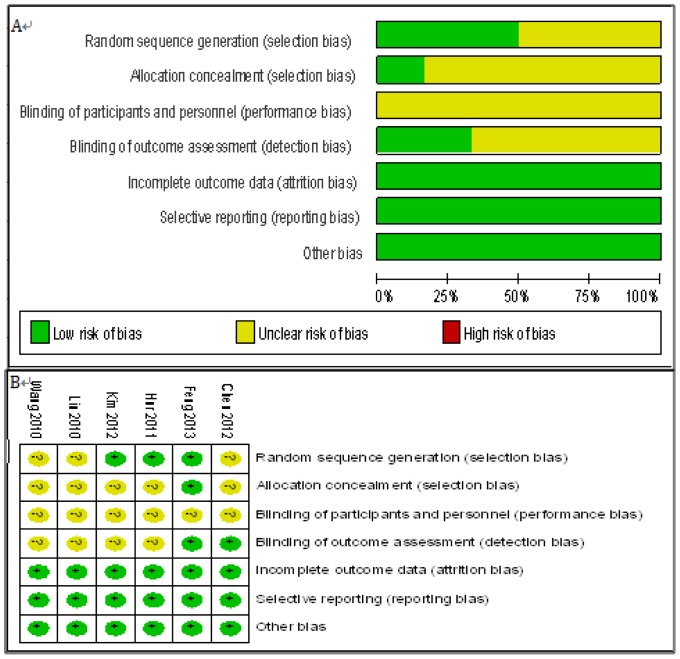
Methods: A literature search in PubMed, Embase, Web of Science and Cochrane library databases was performed for eligible studies published between January 1995 and March 2014. Systematic review was carried out to identify randomized controlled trials comparing EOF and traditional postoperative oral feeding after gastric cancer surgery. Meta-analyses were performed by either a fixed effects model or a random effects model according to the heterogeneity using RevMan 5.2 software.
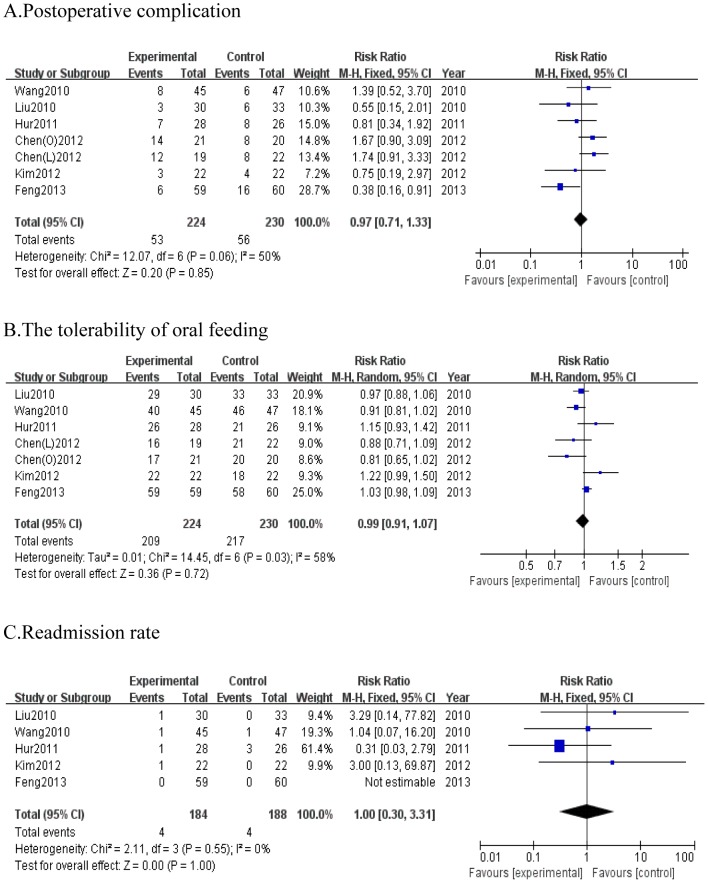
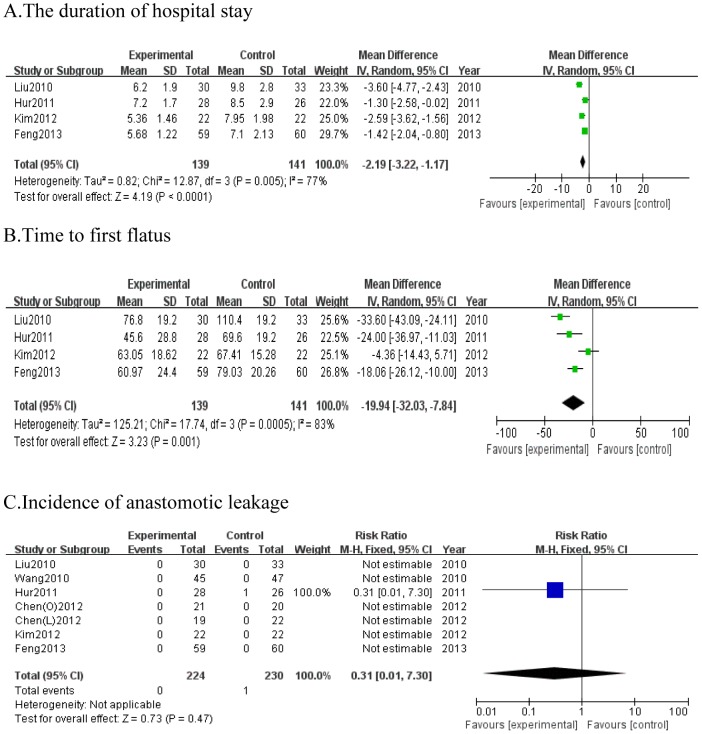
Results: Six studies remained for final analysis. Included studies were published between 2005 and 2013 reporting on a total of 454 patients. No significant differences were observed for postoperative complication (RR = 0.95; 95%CI, 0.70 to 1.29; P = 0.75), the tolerability of oral feeding (RR = 0.98; 95%CI, 0.91 to 1.06; P = 0.61), readmission rate (RR = 1; 95%CI, 0.30 to 3.31; P = 1.00) and incidence of anastomotic leakage (RR = 0.31; 95%CI, 0.01 to 7.30; P = 0.47) between two groups. EOF after gastrectomy for gastric cancer was associated with significant shorter duration of the hospital stay (WMD = -2.36; 95%CI, -3.37 to -1.34; P<0.0001) and time to first flatus (WMD = -19.94; 95%CI, -32.03 to -7.84; P = 0.001). There were no significant differences in postoperative complication, tolerability of oral feeding, readmission rates, duration of hospital stay and time to first flatus among subgroups stratified by the time to start EOF or by partial and total gastrectomy or by laparoscopic and open surgery.
Conclusions: The result of this meta-analysis showed that EOF after gastric cancer surgery seems feasible and safe, even started at the day of surgery irrespective of the extent of the gastric resection and the type of surgery. However, more prospective, well-designed multicenter RCTs with more clinical outcomes are needed for further validation.
Conflict of interest statement
Figures
References
-
- Kehlet H, Wilmore DW (2008) Evidence-based surgical care and the evolution of fast-track surgery. Ann Surg 248: 189–198. - PubMed
-
- Feo CV, Romanini B, Sortini D, Ragazzi R, Zamboni P, et al. (2004) Early oral feeding after colorectal resection: a randomized controlled study. ANZ J Surg 74: 298–301. - PubMed
-
- Zhuang CL, Ye XZ, Zhang CJ, Dong QT, Chen BC, et al. (2013) Early versus traditional postoperative oral feeding in patients undergoing elective colorectal surgery: a meta-analysis of randomized clinical trials. Dig Surg 30: 225–232. - PubMed
-
- Gianotti L, Nespoli L, Torselli L, Panelli M, Nespoli A (2011) Safety, feasibility, and tolerance of early oral feeding after colorectal resection outside an enhanced recovery after surgery (ERAS) program. Int J Colorectal Dis 26: 747–753. - PubMed
-
- de Martel C, Forman D, Plummer M (2013) Gastric cancer: epidemiology and risk factors. Gastroenterol Clin North Am 42: 219–240. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
