

Interhospital Facility Transfers in the United States: A Nationwide Outcomes Study
- PMID: 25397857
- PMCID: PMC4956577
- DOI: 10.1097/PTS.0000000000000148
Interhospital Facility Transfers in the United States: A Nationwide Outcomes Study
Abstract
Objectives: Patient transfers between hospitals are becoming more common in the United States. Disease-specific studies have reported varying outcomes associated with transfer status. However, even as national quality improvement efforts and regulations are being actively adopted, forcing hospitals to become financially accountable for the quality of care provided, surprisingly little is known about transfer patients or their outcomes at a population level. This population-wide study provides timely analyses of the characteristics of this particularly vulnerable and sizable inpatient population. We identified and compared characteristics and outcomes of transfer and nontransfer patients.
Methods: With the use of the 2009 Nationwide Inpatient Sample, a nationally representative sample of U.S. hospitalizations, we examined patient characteristics, in-hospital adverse events, and discharge disposition for transfer versus nontransfer patients in this observational study.
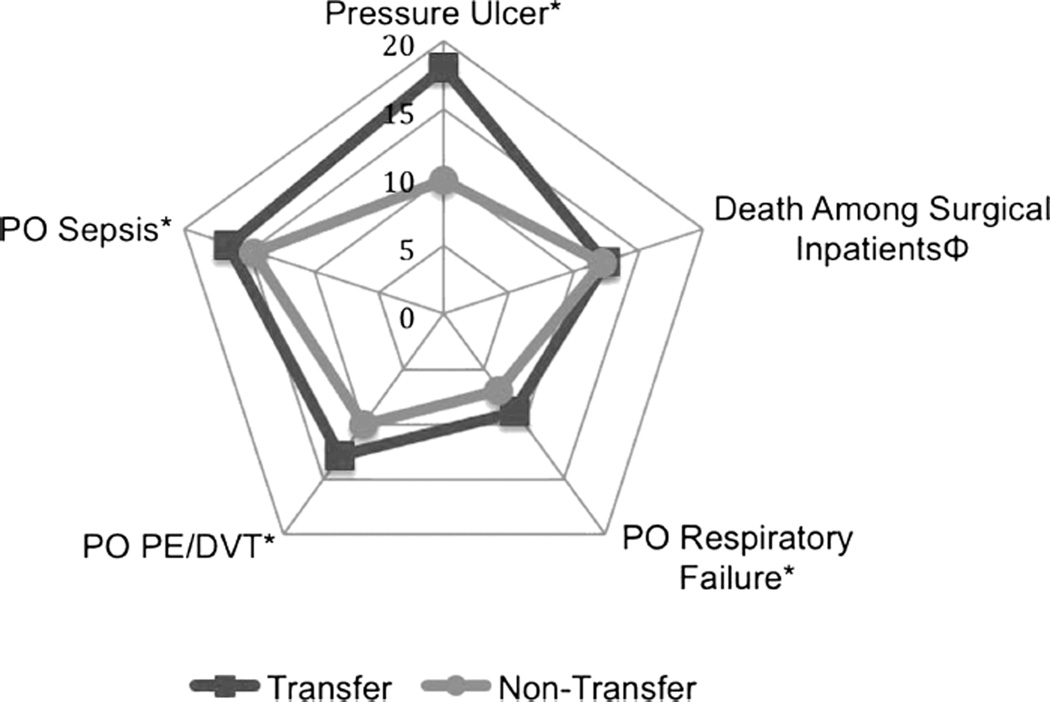
Results: We identified 1,397,712 transfer patients and 31,692,211 nontransfer patients. Age, sex, race, and payer were significantly associated with odds of transfer (P < 0.05). Transfer patients had higher risk-adjusted inpatient mortality (4.6 versus 2.1, P < 0.01), longer length of stay (13.3 versus 4.5, P < 0.01), and fewer routine disposition discharges (53.6 versus 68.7, P < 0.01). In-hospital adverse events were significantly higher in transfer patients compared with nontransfer patients (P < 0.05).
Conclusions: Our results suggest that transfer patients have inferior outcomes compared with nontransfer patients. Although they are clinically complex patients and assessing accountability as between the transferring and receiving hospitals is methodologically difficult, transfer patients must nonetheless be included in quality benchmark data to assess the potential impact this population has on hospital outcome profiles. With hospital accountability and value-based payments constituting an integral part of health care reform, documenting the quality of care delivered to transfer patients is essential before accurate quality assessment improvement efforts can begin in this patient population.
Conflict of interest statement
The authors disclose no conflict of interest.
Figures
Similar articles
-
Discharge dispositions, complications, and costs of hospitalization in spinal cord tumor surgery: analysis of data from the United States Nationwide Inpatient Sample, 2003-2010.J Neurosurg Spine. 2014 Feb;20(2):125-41. doi: 10.3171/2013.9.SPINE13274. Epub 2013 Nov 29. J Neurosurg Spine. 2014. PMID: 24286530
-
Impact of transfer status on hospitalization cost and discharge disposition for acute ischemic stroke across the US.J Neurosurg. 2016 May;124(5):1228-37. doi: 10.3171/2015.4.JNS141631. Epub 2015 Oct 9. J Neurosurg. 2016. PMID: 26452123
-
Observed and expected outcomes in transfer and nontransfer patients with a hip fracture.J Orthop Trauma. 2011 Nov;25(11):666-9. doi: 10.1097/BOT.0b013e31821146b1. J Orthop Trauma. 2011. PMID: 21857540
-
Outcomes of Ventilated Patients With Sepsis Who Undergo Interhospital Transfer: A Nationwide Linked Analysis.Crit Care Med. 2018 Jan;46(1):e81-e86. doi: 10.1097/CCM.0000000000002777. Crit Care Med. 2018. PMID: 29068858 Free PMC article.
-
Optimizing Safety for Surgical Patients Undergoing Interhospital Transfer.Surg Clin North Am. 2021 Feb;101(1):57-69. doi: 10.1016/j.suc.2020.09.002. Epub 2020 Nov 2. Surg Clin North Am. 2021. PMID: 33212080 Review.
Cited by
-
Differences in Interfacility Transfer from Emergency Department and Inpatient Services for Inpatient Neurologic Care.Neurohospitalist. 2024 Oct;14(4):406-412. doi: 10.1177/19418744241273205. Epub 2024 Aug 13. Neurohospitalist. 2024. PMID: 39308471
-
Physician Perspectives on Interhospital Transfers.J Patient Saf. 2019 Jun;15(2):86-89. doi: 10.1097/PTS.0000000000000312. J Patient Saf. 2019. PMID: 27811599 Free PMC article.
-
Rates, Predictors and Variability of Interhospital Transfers: A National Evaluation.J Hosp Med. 2017 Jun;12(6):435-442. doi: 10.12788/jhm.2747. J Hosp Med. 2017. PMID: 28574533 Free PMC article.
-
Implications of interhospital patient transfers for emergency medical services transportation systems in the Netherlands: a retrospective study.BMJ Open. 2024 Jun 13;14(6):e077181. doi: 10.1136/bmjopen-2023-077181. BMJ Open. 2024. PMID: 38871665 Free PMC article.
-
Association of transfer time and delays with outcomes for patients with acute pulmonary embolism requiring interhospital transfer: a retrospective observational study.Ann Med. 2025 Dec;57(1):2534094. doi: 10.1080/07853890.2025.2534094. Epub 2025 Jul 25. Ann Med. 2025. PMID: 40711763 Free PMC article.
References
-
- Steiner C, Elixhauser A, Schnaier J. The Healthcare Cost and Utilization Project: an overview. Eff Clin Pract. 2002;5:143–151. - PubMed
-
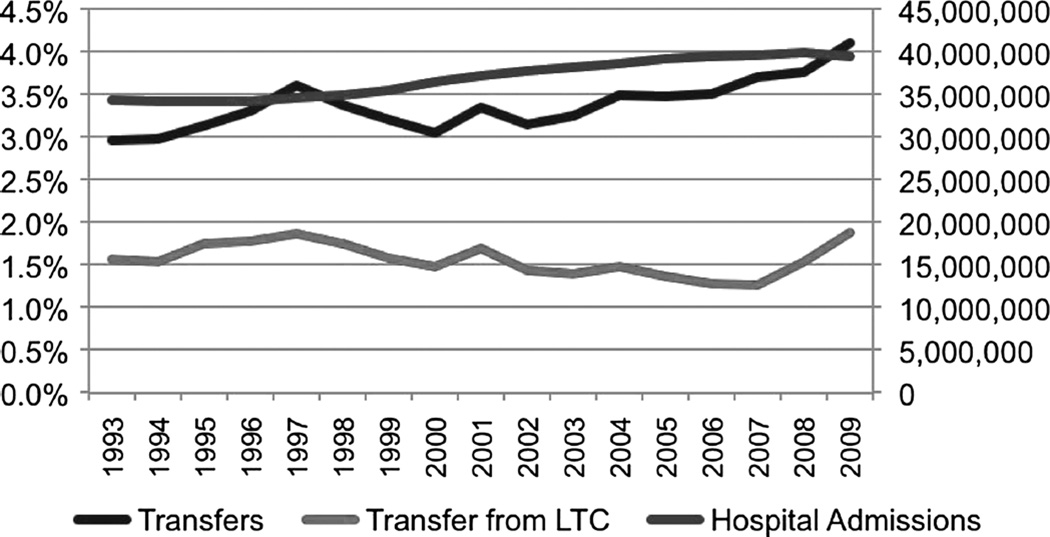
- Rockville, MD: Agency for Healthcare Research and Quality; [Accessed February 22, 2013]. HCUPnet. Healthcare Cost and Utilization Project (HCUP). 1993–2011. http://hcupnet.ahrq.gov/ - PubMed
-
- Munoz E, Soldano R, Gross H, et al. Diagnosis related groups and the transfer of general surgical patients between hospitals. Arch Surg. 1988;123:68–71. - PubMed
-
- Borlase BC, Baxter JT, Benotti PN, et al. Surgical intensive care unit resource use in a specialty referral hospital: I. Predictors of early death and cost implications. Surgery. 1991;109:687–693. - PubMed
-
- Human and Health Services, editor. Healthcare Cost and Utilization Project. Facts and Figures 2009. Rockville, MD: Agency for Healthcare Research & Quality; 2011.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
