

Sex differences in patients receiving anticoagulant therapy for venous thromboembolism
- PMID: 25398066
- PMCID: PMC4602415
- DOI: 10.1097/MD.0000000000000114
Sex differences in patients receiving anticoagulant therapy for venous thromboembolism
Abstract
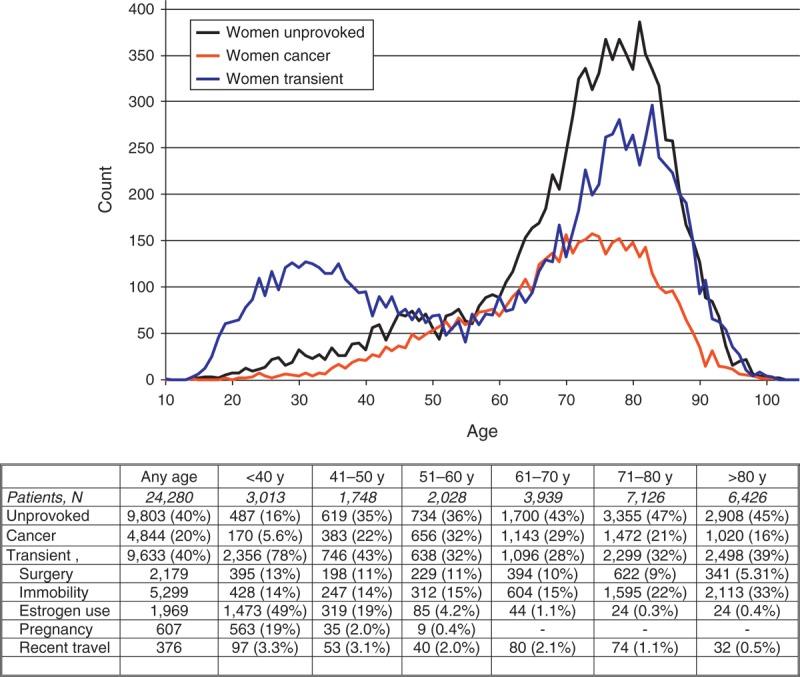
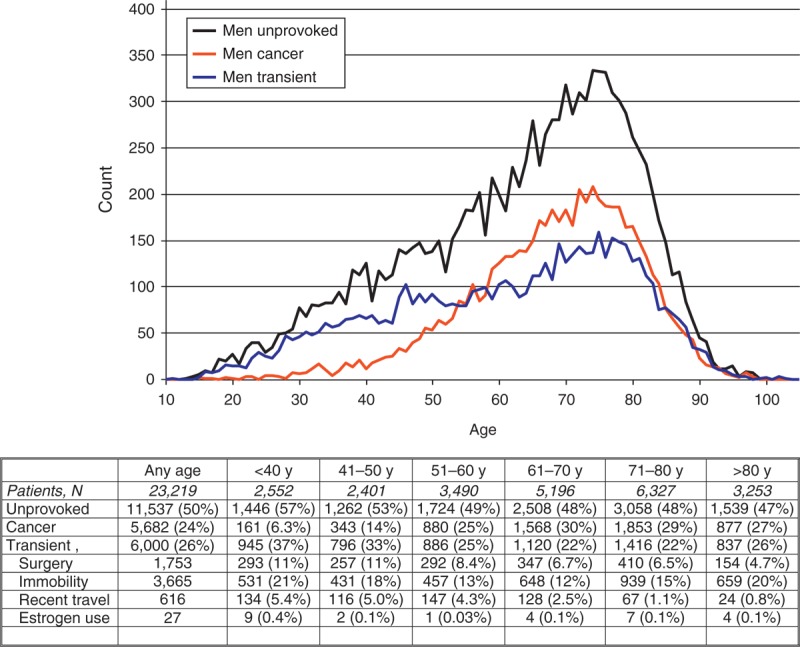
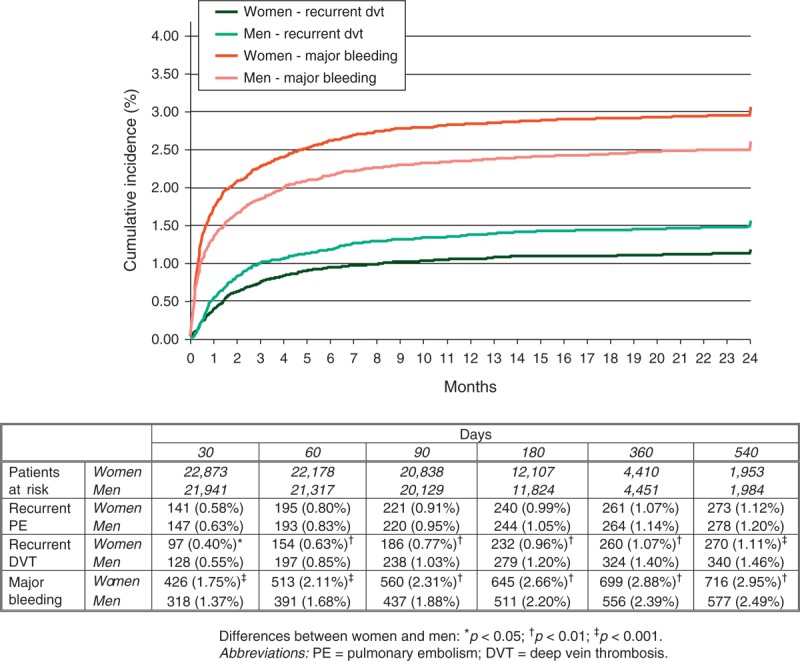
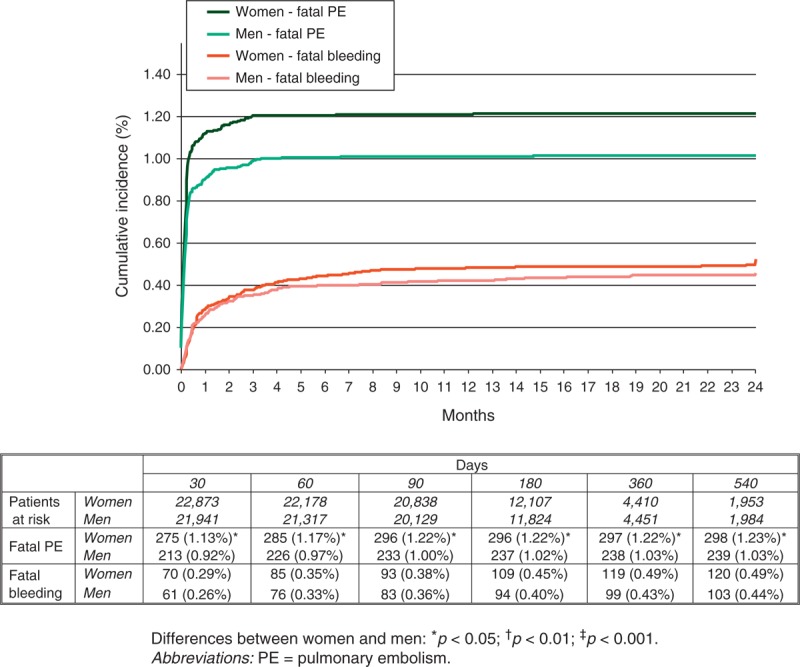
In patients with venous thromboembolism (VTE), the outcome during the course of anticoagulant therapy may differ according to the patient's sex. We used the RIETE (Registro Informatizado Enfermedad TromboEmbólica) database to compare the rate of VTE recurrences, major bleeding, and mortality due to these events according to sex.As of August 2013, 47,499 patients were enrolled in RIETE, of whom 24,280 (51%) were women. Women were older, more likely presented with pulmonary embolism (PE), and were more likely to have recent immobilization but less likely to have cancer than men. During the course of anticoagulation (mean duration: 253 d), 659 patients developed recurrent deep vein thrombosis (DVT), 576 recurrent PE, 1368 bled, and 4506 died. Compared with men, women had a lower rate of DVT recurrences (hazard ratio [HR]: 0.78; 95% confidence interval [CI]: 0.67-0.91), a similar rate of PE recurrences (HR: 0.98; 95% CI: 0.83-1.15), a higher rate of major bleeding (HR: 1.21; 95% CI: 1.09-1.35), and higher mortality due to PE (HR: 1.24; 95% CI: 1.04-1.47). On multivariable analysis, any influence of sex on the risk for recurrent DVT (HR: 0.88; 95% CI: 0.75-1.03), major bleeding (HR: 1.10; 95% CI: 0.98-1.24), or fatal PE (HR: 1.01; 95% CI: 0.84-1.22) was no longer statistically significant.In conclusion, women had fewer DVT recurrences and more bleeds than men during the course of anticoagulation. These differences were not due to sex, but very likely to other patient characteristics more common in female patients and differences in treatment choice.
Conflict of interest statement
Financial support and conflicts of interest: Sanofi Spain supported the Registry with an unrestricted educational grant, and Bayer Pharma AG supported the part of RIETE Registry outside Spain, which accounts for 19.1% of the total patients included in the RIETE Registry.
Figures
References
-
- Agnelli G, Buller HR, Cohen A, et al. For the AMPLIFY Investigators. N Engl J Med. 2013;369:799–808. - PubMed
-
- Agnelli G, Prandoni P, Becattini C, et al. Extended oral anticoagulant therapy after a first episode of pulmonary embolism. Ann Intern Med. 2003;139:19–25. - PubMed
-
- Agnelli G, Prandoni P, Santamaria MG, et al. Three months versus one year of oral anticoagulant therapy for idiopathic deep venous thrombosis. Warfarin optimal Duration Italian Trial Investigators. N Engl J Med. 2001;345:165–169. - PubMed
-
- Baglin T, Luddington R, Brown K, et al. High risk of recurrent venous thromboembolism in men. J Thromb Haemost. 2004;2:2152–2155. - PubMed
-
- Christiansen SC, Lijfering WM, Helmerhorst FM, et al. Sex difference in risk of recurrent venous thrombosis and the risk profile for a second event. J Thromb Haemost. 2010;8:2159–2168. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
