

Oncolytic measles virus expressing the sodium iodide symporter to treat drug-resistant ovarian cancer
- PMID: 25398436
- PMCID: PMC4377302
- DOI: 10.1158/0008-5472.CAN-14-2533
Oncolytic measles virus expressing the sodium iodide symporter to treat drug-resistant ovarian cancer
Abstract
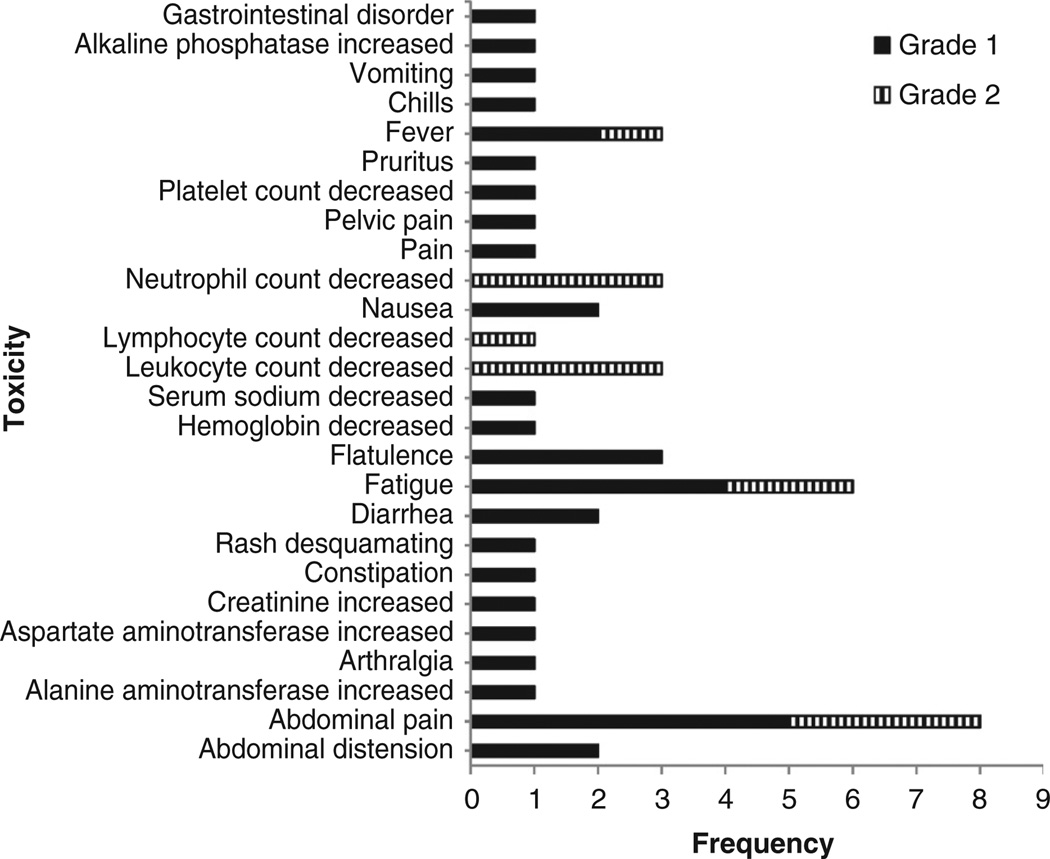
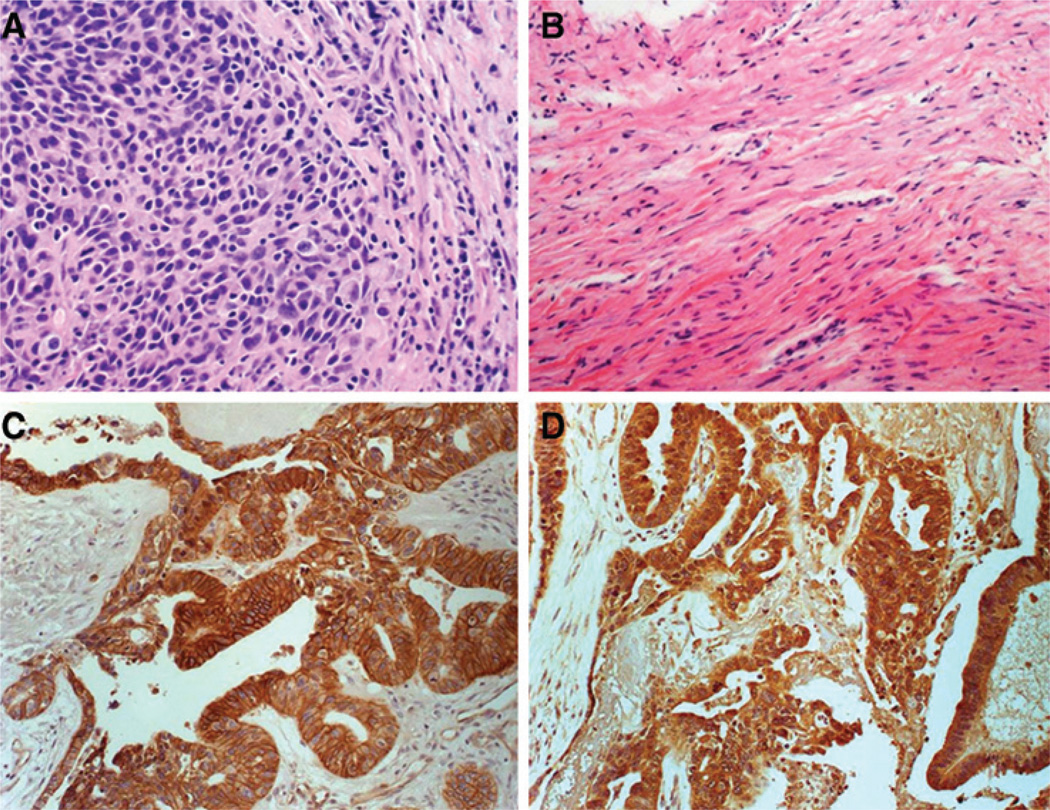
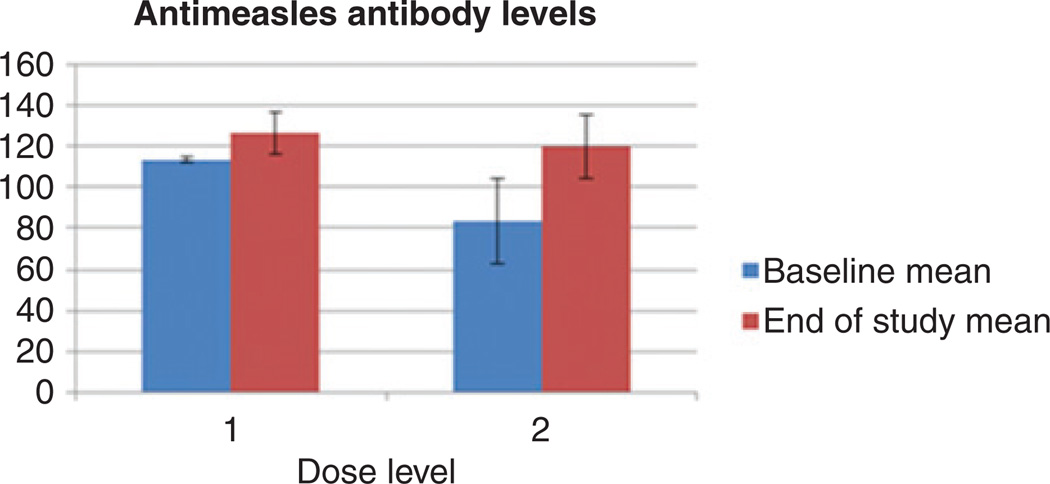
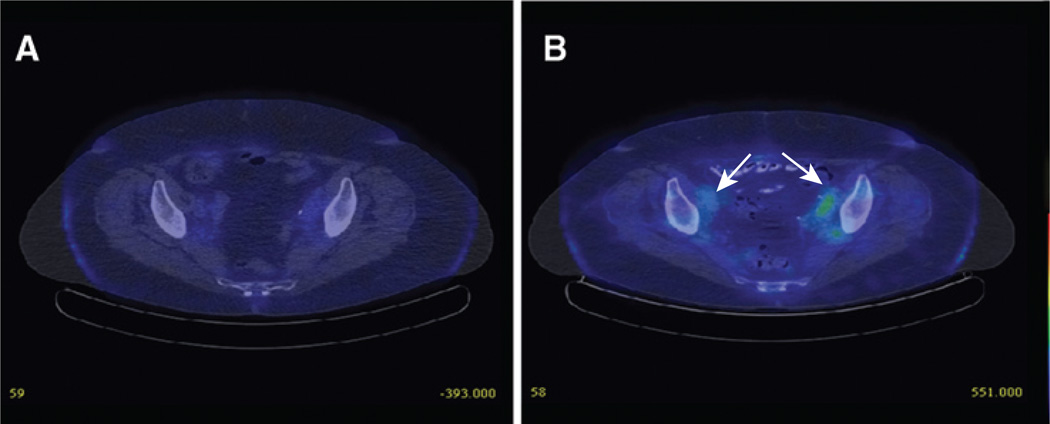
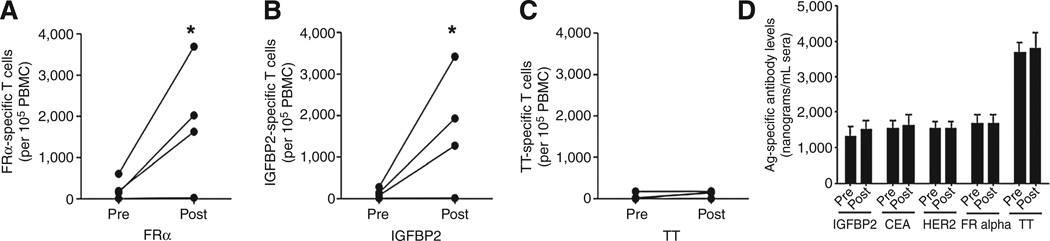
Edmonston vaccine strains of measles virus (MV) have significant antitumor activity in mouse xenograft models of ovarian cancer. MV engineered to express the sodium iodide symporter gene (MV-NIS) facilitates localization of viral gene expression and offers a tool for tumor radiovirotherapy. Here, we report results from a clinical evaluation of MV-NIS in patients with taxol- and platinum-resistant ovarian cancer. MV-NIS was given intraperitoneally every 4 weeks for up to 6 cycles. Treatment was well tolerated and associated with promising median overall survival in these patients with heavily pretreated ovarian cancer; no dose-limiting toxicity was observed in 16 patients treated at high-dose levels (10(8)-10(9) TCID50), and their median overall survival of 26.5 months compared favorably with other contemporary series. MV receptor CD46 and nectin-4 expression was confirmed by immunohistochemistry in patient tumors. Sodium iodide symporter expression in patient tumors after treatment was confirmed in three patients by (123)I uptake on SPECT/CTs and was associated with long progression-free survival. Immune monitoring posttreatment showed an increase in effector T cells recognizing the tumor antigens IGFBP2 and FRα, indicating that MV-NIS treatment triggered cellular immunity against the patients' tumor and suggesting that an immune mechanism mediating the observed antitumor effect. Our findings support further clinical evaluation of MV-NIS as an effective immunovirotherapy.
©2014 American Association for Cancer Research.
Conflict of interest statement
M.J. Federspiel has ownership interest (including patents) in Magnis Therapeutics LLC. S.J. Russell is CEO and has ownership interest (including patents) in Magnis Therapeutics LLC. No potential conflicts of interest were disclosed by the other authors.
Figures
References
-
- Siegel R, Ma J, Zou Z, Jemal A. Cancer Statistics, 2014. CA Cancer J Clin. 2014;64:9–29. - PubMed
-
- Ferrandina G, Ludovisi M, Lorusso D, Pignata S, Breda E, Savarese A, et al. Phase III trial of gemcitabine compared with pegylated liposomal doxorubicin in progressive or recurrent ovarian cancer. J Clin Oncol. 2008;26:890–896. - PubMed
-
- Vergote I, Finkler N, del Campo J, Lohr A, Hunter J, Matei D, et al. Phase 3 randomised study of canfosfamide (Telcyta, TLK286) versus pegylated liposomal doxorubicin or topotecan as third-line therapy in patients with platinum-refractory or -resistant ovarian cancer. Eur J Cancer. 2009;45:2324–2332. - PubMed
-
- Lamb RA, Kolakofsky D, editors. Paramyxoviridae: the viruses and their replication. 4th ed. Philadelphia, PA: Lippincott-Raven Publishers; 2001.
-
- Markman M, Blessing J, Rubin SC, Connor J, Hanjani P, Waggoner S. Phase II trial of weekly paclitaxel (80mg/m2) in platinum and paclitaxel-resistant ovarian and primary peritoneal cancers: a Gynecologic Oncology Group study. Gynecol Oncol. 2006;101:436–440. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
