

Actual versus ideal body weight for acute kidney injury diagnosis and classification in critically ill patients
- PMID: 25398596
- PMCID: PMC4236495
- DOI: 10.1186/1471-2369-15-176
Actual versus ideal body weight for acute kidney injury diagnosis and classification in critically ill patients
Abstract
Background: In the current acute kidney injury (AKI) definition, the urine output (UO) criterion does not specify which body weights (BW), i.e. actual (ABW) versus ideal (IBW), should be used to diagnose and stage AKI, leading to heterogeneity across research studies.
Methods: This is a single center, retrospective, observational study conducted at a tertiary referral hospital. All adult patients who were admitted to intensive care units (ICUs) at our institution for a minimum of 6 continuous hours between January and March 2010 and had a urinary catheter for hourly urine output monitoring were eligible for this study. Patients' AKI stages, based on UO criterion, were assessed by calculating each milliliter of urine per kilogram per hour, using ABW versus IBW.
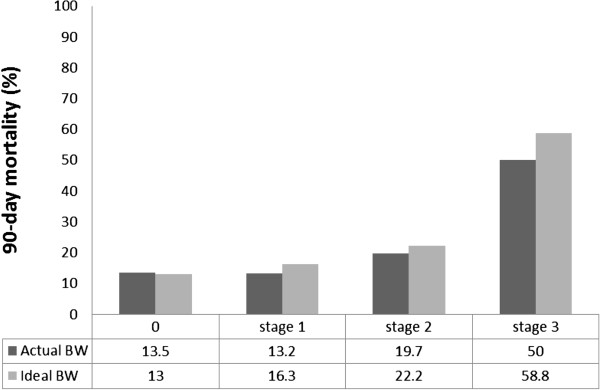
Results: A total of 493 ICU patients were included in the analysis. The median ABW and IBW were 82 (IQR 68-96) and 70 (IQR 60-77) kg, respectively. Using the IBW criterion, 154 patients (31.2%) were diagnosed with AKI, while 204 (41.4%) were diagnosed using the ABW measurement (P-value<.01). Patients who had AKI regardless of BW type had an adjusted odds ratio of 1.76 (95% CI 1.05-2.95) for 90-day mortality, whereas patients who had AKI according to ABW but not IBW had no significant increase in the risk of 90-day mortality, adjusted OR 0.76; (95% CI 0.25-1.91), compared to patients who had no AKI.
Conclusions: Using ABW to diagnose and stage AKI by UO criterion is more sensitive and less specific than IBW. Based on the application of the definition, different BW types could be utilized.
Figures
References
Pre-publication history
-
- The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2369/15/176/prepub
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
