

Immunotherapy for primary brain tumors: no longer a matter of privilege
- PMID: 25398845
- PMCID: PMC4235630
- DOI: 10.1158/1078-0432.CCR-14-0832
Immunotherapy for primary brain tumors: no longer a matter of privilege
Abstract
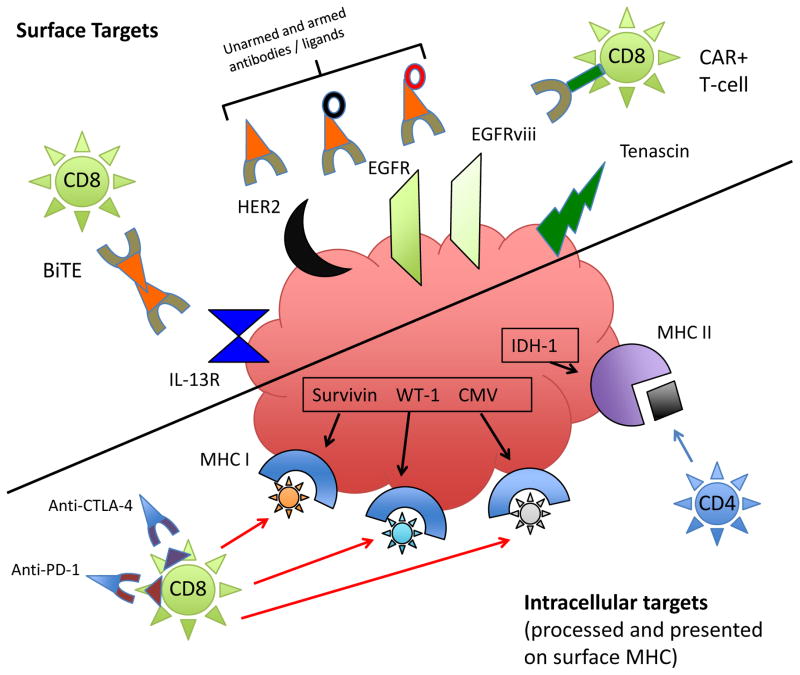
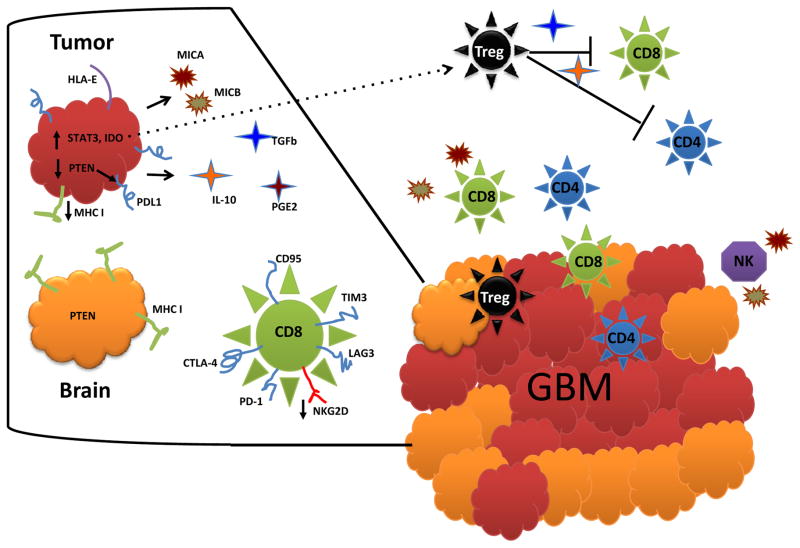
Immunotherapy for cancer continues to gain both momentum and legitimacy as a rational mode of therapy and a vital treatment component in the emerging era of personalized medicine. Gliomas, and their most malignant form, glioblastoma, remain as a particularly devastating solid tumor for which standard treatment options proffer only modest efficacy and target specificity. Immunotherapy would seem a well-suited choice to address such deficiencies given both the modest inherent immunogenicity of gliomas and the strong desire for treatment specificity within the confines of the toxicity-averse normal brain. This review highlights the caveats and challenges to immunotherapy for primary brain tumors, as well as reviewing modalities that are currently used or are undergoing active investigation. Tumor immunosuppressive countermeasures, peculiarities of central nervous system immune access, and opportunities for rational treatment design are discussed.
©2014 American Association for Cancer Research.
Conflict of interest statement
J.H. Sampson is a consultant/advisory board member for CellDex Therapeutics, and reports receiving a commercial research grant and licensing fees from CellDex Therapeutics for intellectual property related to the EGFRvIII peptide vaccine (CDX-110). A.B. Heimberger is a consultant/advisory board member for Bristol-Myers Squibb; holds patents on WP1066 and the immune modulatory miRNA portfolios; reports receiving a research grant from Merck and licensing fees from CellDex Therapeutics for intellectual property related to the EGFRvIII peptide vaccine (CDX-110). No potential conflicts of interest were disclosed by the other author.
Figures
References
-
- Kantoff PW, Higano CS, Shore ND, Berger ER, Small EJ, Penson DF, et al. Sipuleucel-T immunotherapy for castration-resistant prostate cancer. N Engl J Med. 2010;363:411–22. - PubMed
-
- Dunn GP, Fecci PE, Curry WT. Cancer immunoediting in malignant glioma. Neurosurgery. 2012;71(2):201–23. - PubMed
-
- Cserr HF, Knopf PM. Cervical lymphatics, the blood-brain barrier and the immunoreactivity of the brain: a new view. Immunol Today. 1992;13:507–12. - PubMed
-
- Cserr HF, Harling-Berg CJ, Knopf PM. Drainage of brain extracellular fluid into blood and deep cervical lymph and its immunological significance. Brain Pathol. 1992;2:269–76. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
