

How we treat chronic graft-versus-host disease
- PMID: 25398933
- PMCID: PMC4304105
- DOI: 10.1182/blood-2014-08-551994
How we treat chronic graft-versus-host disease
Abstract
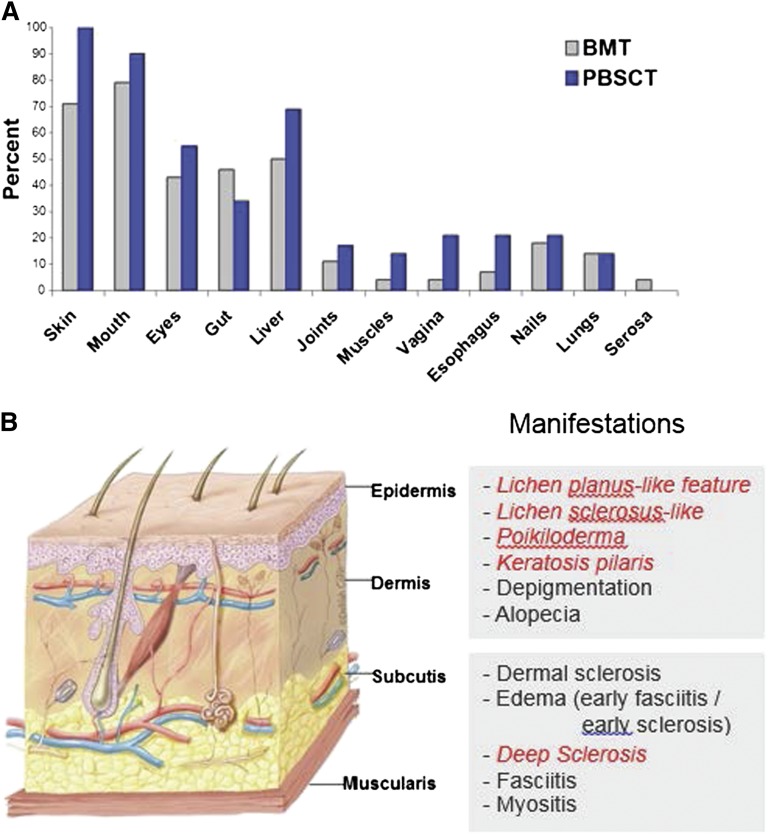
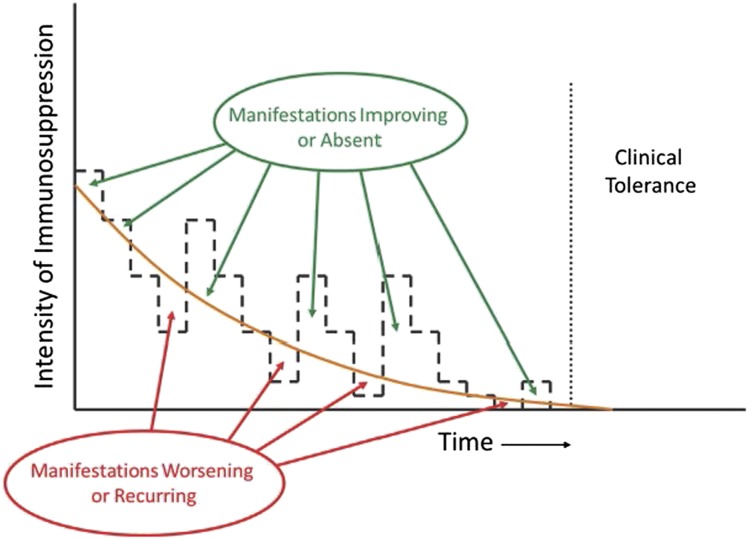
Chronic graft-versus-host disease (GVHD) remains a common and potentially life-threatening complication of allogeneic hematopoietic stem cell transplantation (HCT). The 2-year cumulative incidence of chronic GVHD requiring systemic treatment is ~30% to 40% by National Institutes of Health criteria. The risk of chronic GVHD is higher and the duration of treatment is longer after HCT with mobilized blood cells than with marrow cells. Clinical manifestations can impair activities of daily living and often linger for years. Hematology and oncology specialists who refer patients to centers for HCT are often subsequently involved in the management of chronic GVHD when patients return to their care after HCT. Treatment of these patients can be optimized under shared care arrangements that enable referring physicians to manage long-term administration of immunosuppressive medications and supportive care with guidance from transplant center experts. Keys to successful collaborative management include early recognition in making the diagnosis of chronic GVHD, comprehensive evaluation at the onset and periodically during the course of the disease, prompt institution of systemic and topical treatment, appropriate monitoring of the response, calibration of treatment intensity over time in order to avoid overtreatment or undertreatment, and the use of supportive care to prevent complications and disability.
© 2015 by The American Society of Hematology.
Figures
References
-
- Center for International Blood and Marrow Transplant Research. CIBMTR 2014. http://www.cibmtr.org. Accessed August 5, 2014.
-
- Lee SJ, Vogelsang G, Flowers ME. Chronic graft-versus-host disease. Biol Blood Marrow Transplant. 2003;9(4):215–233. - PubMed
-
- Flowers ME, Parker PM, Johnston LJ, et al. Comparison of chronic graft-versus-host disease after transplantation of peripheral blood stem cells versus bone marrow in allogeneic recipients: long-term follow-up of a randomized trial. Blood. 2002;100(2):415–419. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
