

Assessment-driven selection and adaptation of exercise difficulty in robot-assisted therapy: a pilot study with a hand rehabilitation robot
- PMID: 25399249
- PMCID: PMC4273449
- DOI: 10.1186/1743-0003-11-154
Assessment-driven selection and adaptation of exercise difficulty in robot-assisted therapy: a pilot study with a hand rehabilitation robot
Abstract
Background: Selecting and maintaining an engaging and challenging training difficulty level in robot-assisted stroke rehabilitation remains an open challenge. Despite the ability of robotic systems to provide objective and accurate measures of function and performance, the selection and adaptation of exercise difficulty levels is typically left to the experience of the supervising therapist.
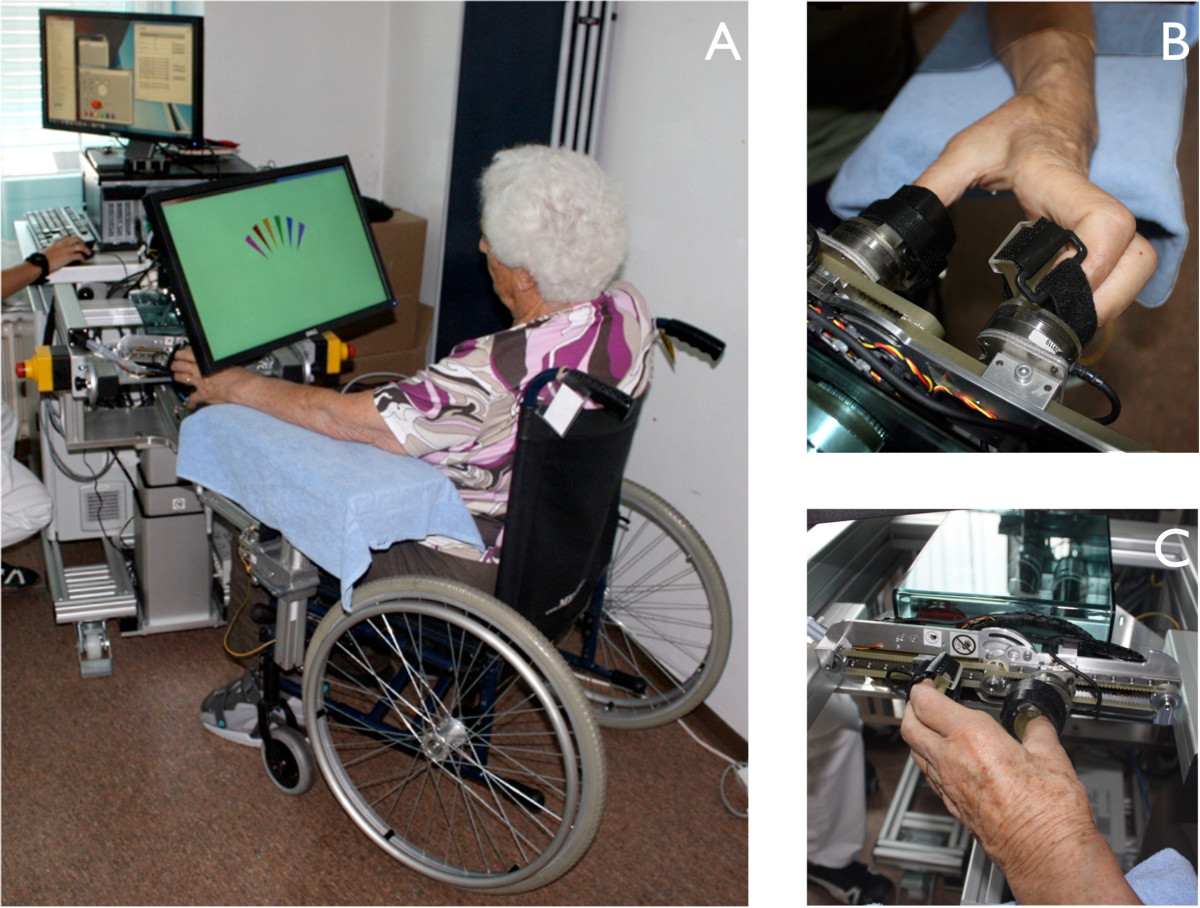
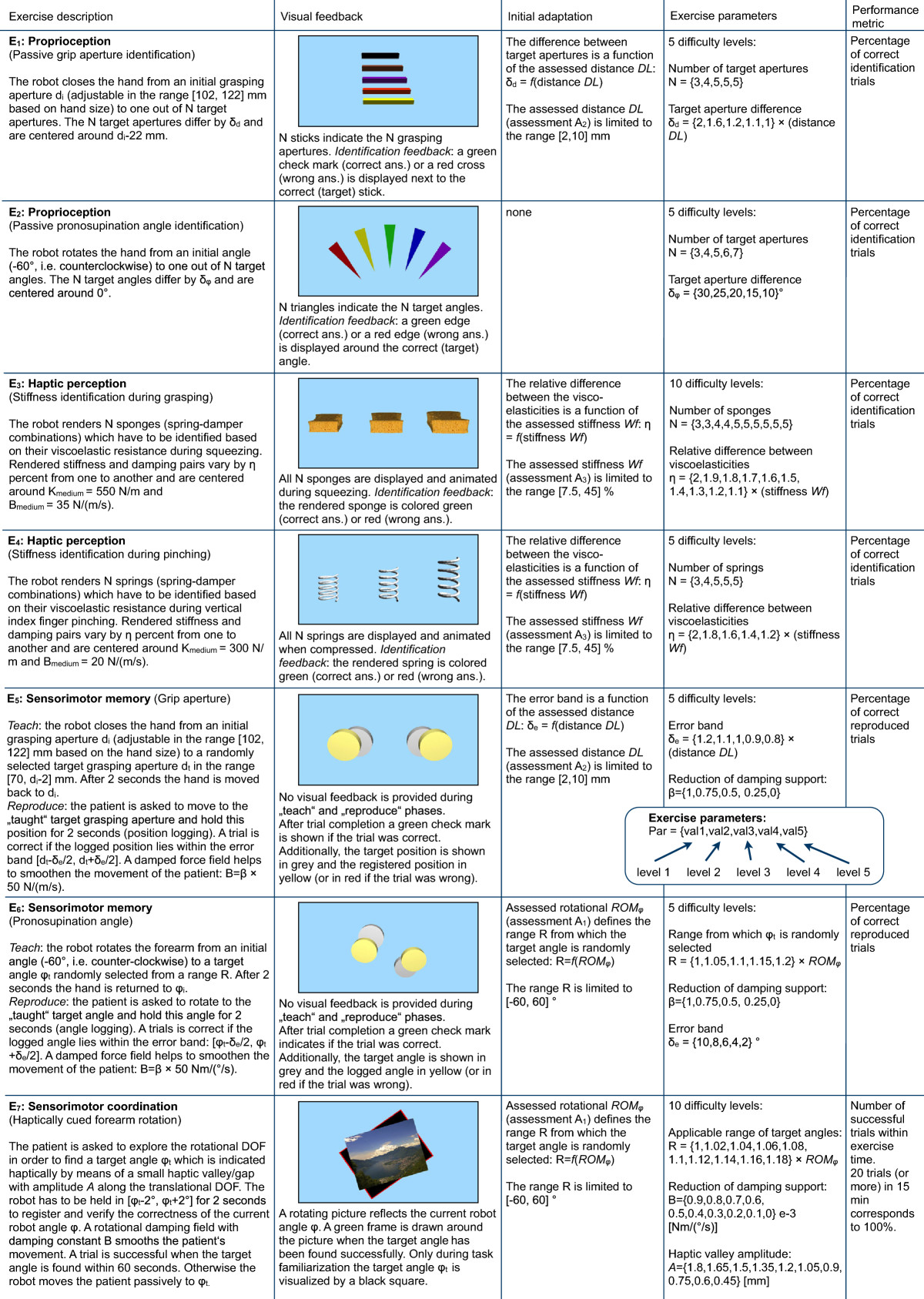
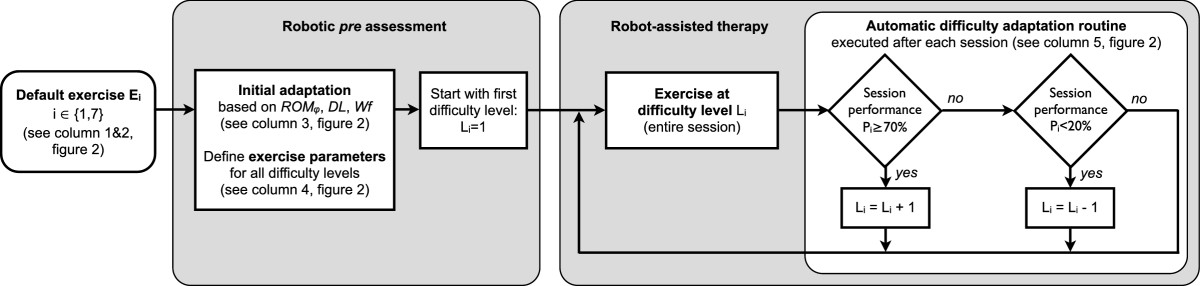
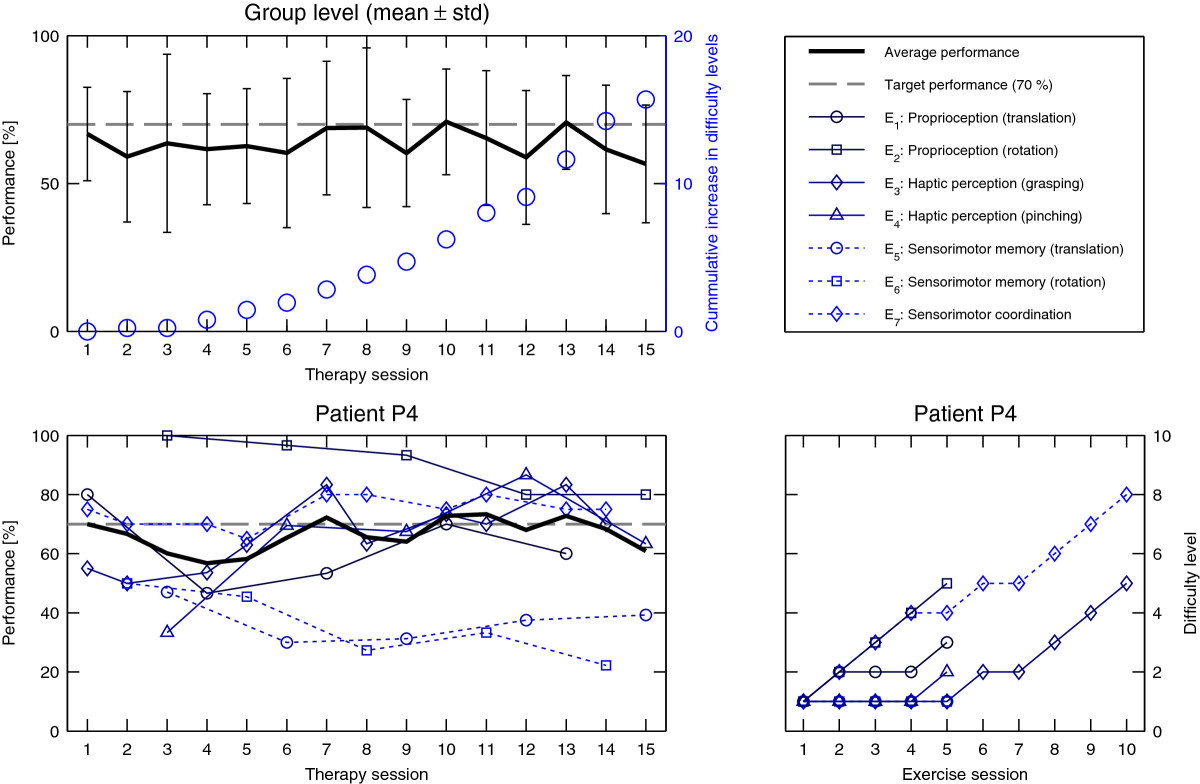
Methods: We introduce a patient-tailored and adaptive robot-assisted therapy concept to optimally challenge patients from the very first session and throughout therapy progress. The concept is evaluated within a four-week pilot study in six subacute stroke patients performing robot-assisted rehabilitation of hand function. Robotic assessments of both motor and sensory impairments of hand function conducted prior to the therapy are used to adjust exercise parameters and customize difficulty levels. During therapy progression, an automated routine adapts difficulty levels from session to session to maintain patients' performance around a target level of 70%, to optimally balance motivation and challenge.
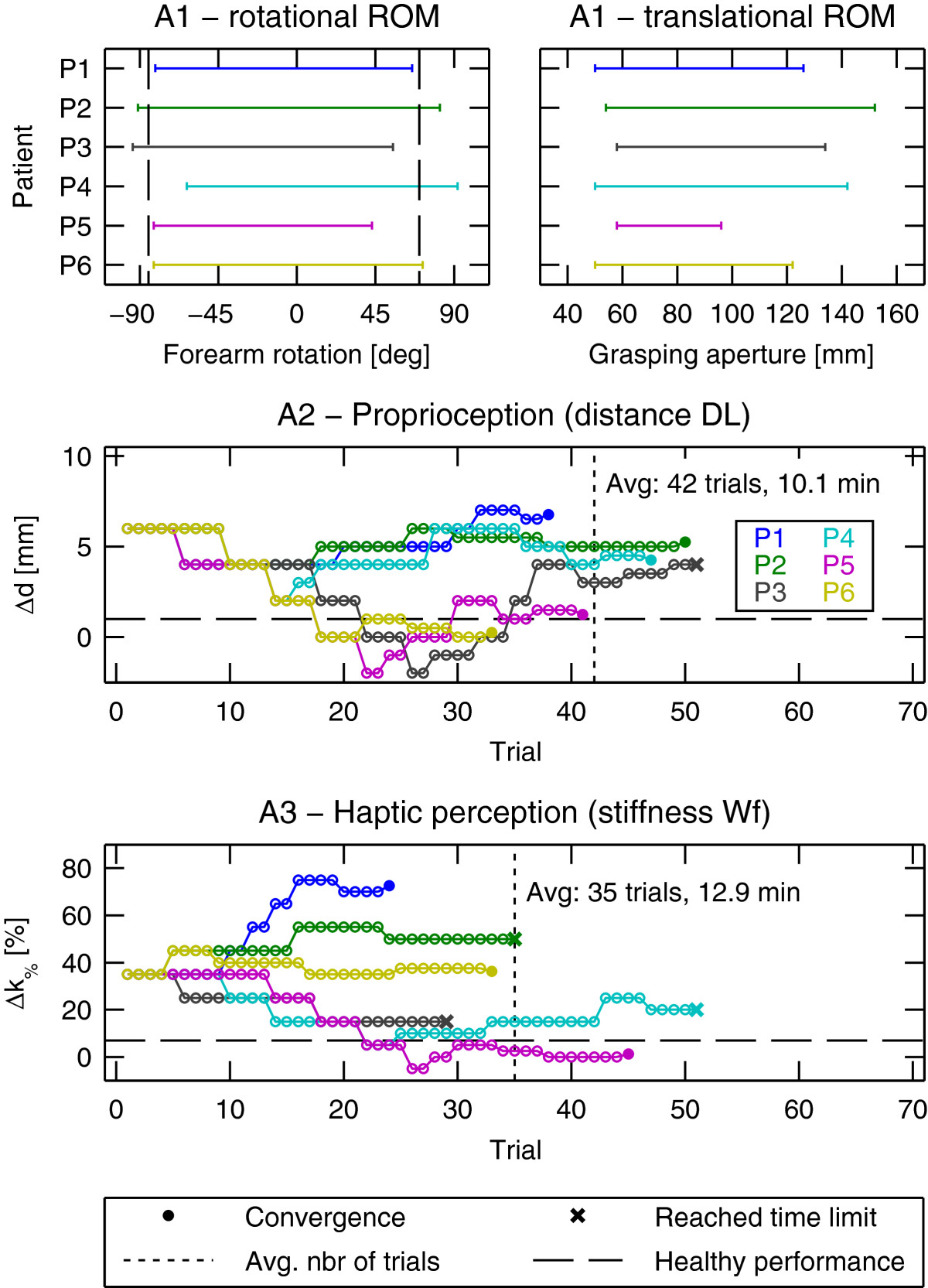
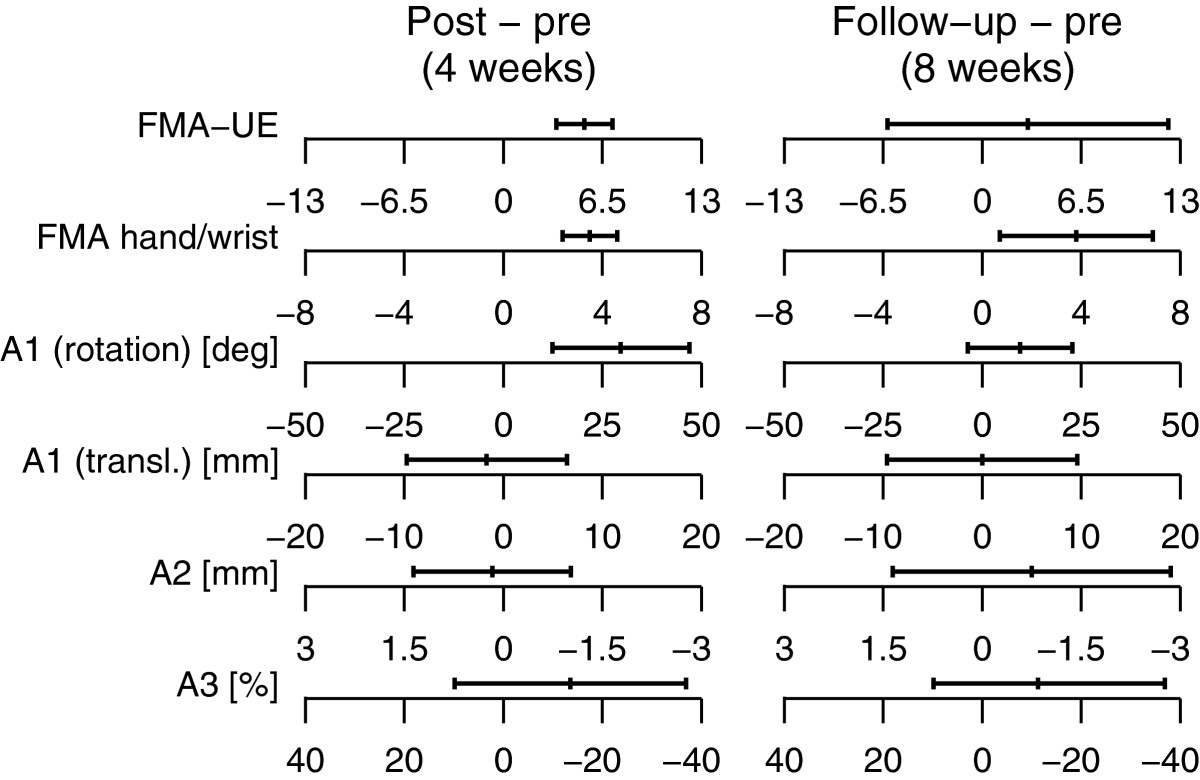
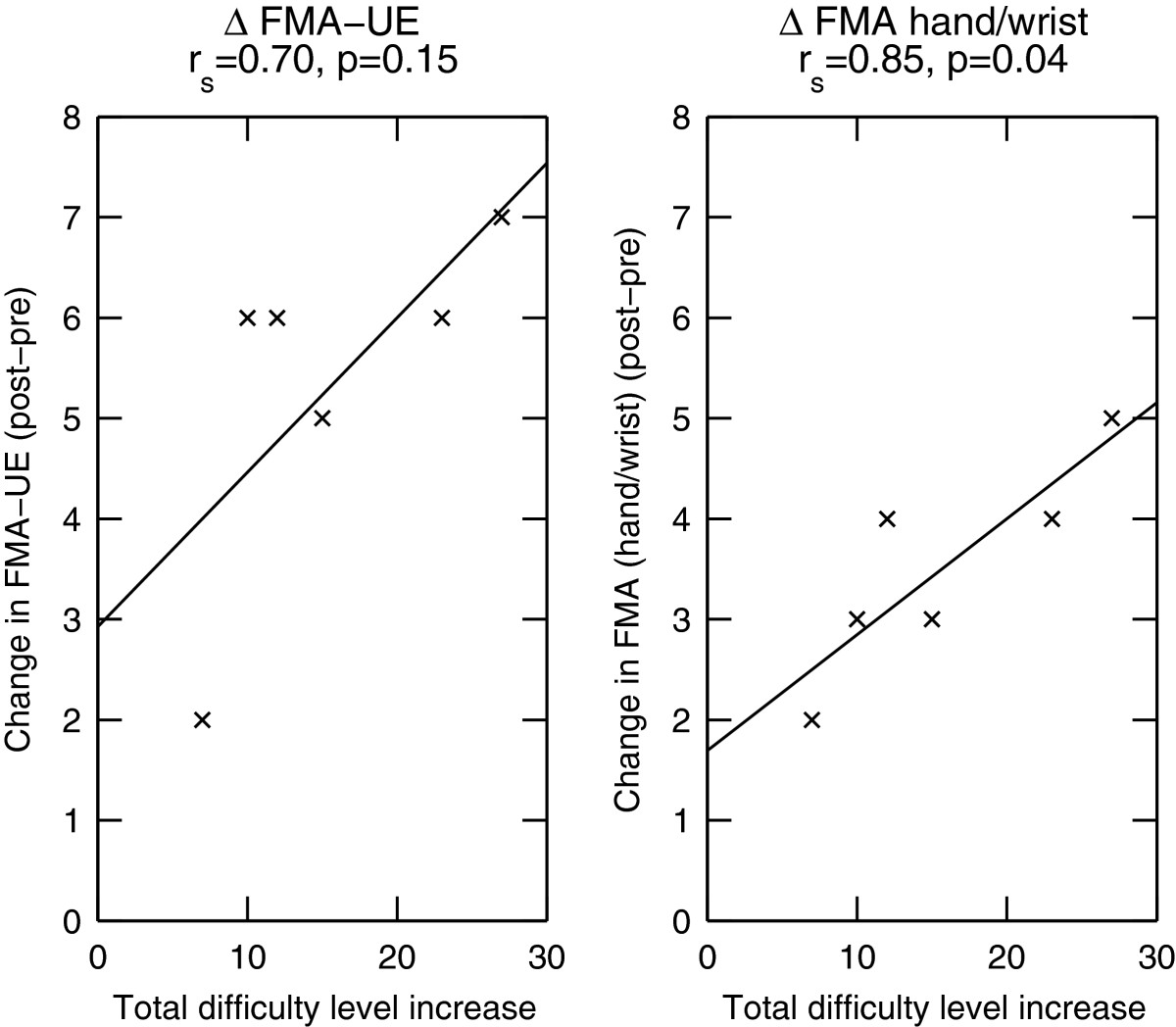
Results: Robotic assessments suggested large differences in patients' sensorimotor abilities that are not captured by clinical assessments. Exercise customization based on these assessments resulted in an average initial exercise performance around 70% (62% ± 20%, mean ± std), which was maintained throughout the course of the therapy (64% ± 21%). Patients showed reduction in both motor and sensory impairments compared to baseline as measured by clinical and robotic assessments. The progress in difficulty levels correlated with improvements in a clinical impairment scale (Fugl-Meyer Assessment) (r s = 0.70), suggesting that the proposed therapy was effective at reducing sensorimotor impairment.
Conclusions: Initial robotic assessments combined with progressive difficulty adaptation have the potential to automatically tailor robot-assisted rehabilitation to the individual patient. This results in optimal challenge and engagement of the patient, may facilitate sensorimotor recovery after neurological injury, and has implications for unsupervised robot-assisted therapy in the clinic and home environment.
Trial registration: ClinicalTrials.gov, NCT02096445.
Figures
References
-
- Duncan P. Synthesis of intervention trials to improve motor recovery following stroke. Topics Stroke Rehabil. 1997;3:1–20. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
