

Recent trends in survival from out-of-hospital cardiac arrest in the United States
- PMID: 25399396
- PMCID: PMC4276415
- DOI: 10.1161/CIRCULATIONAHA.114.009711
Recent trends in survival from out-of-hospital cardiac arrest in the United States
Abstract
Background: Despite intensive efforts over many years, the United States has made limited progress in improving rates of survival from out-of-hospital cardiac arrest. Recently, national organizations, such as the American Heart Association, have focused on promoting bystander cardiopulmonary resuscitation, use of automated external defibrillators, and other performance improvement efforts.
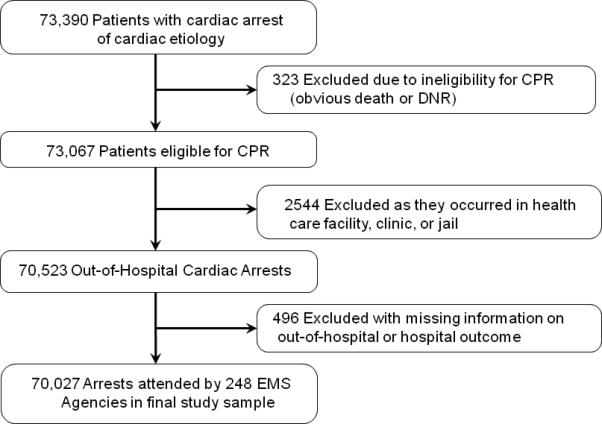
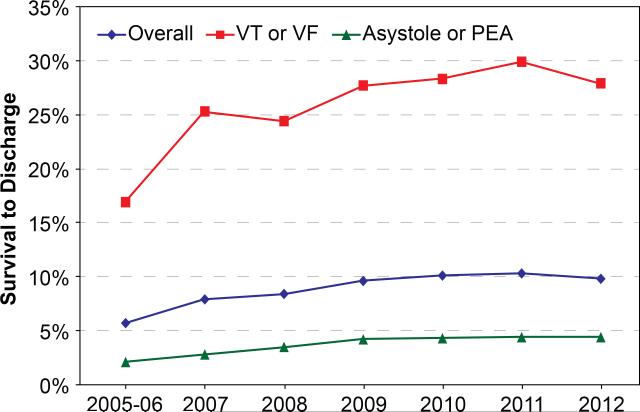
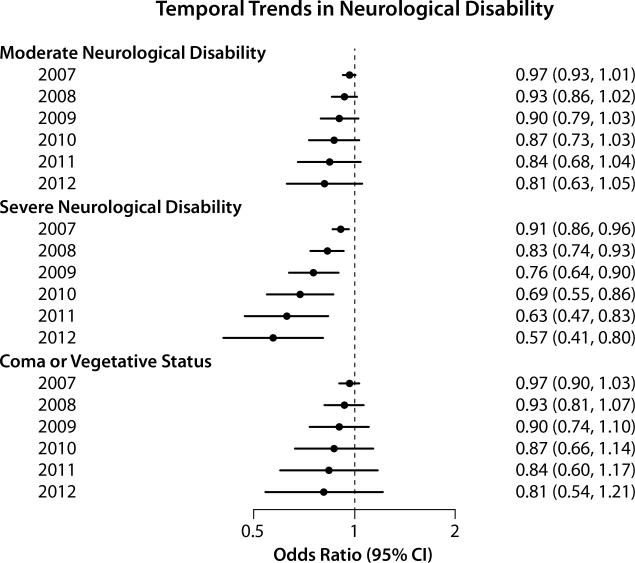
Methods and results: Using the Cardiac Arrest Registry to Enhance Survival (CARES), a prospective clinical registry, we identified 70 027 U.S. patients who experienced an out-of-hospital cardiac arrest between October 2005 and December 2012. Using multilevel Poisson regression, we examined temporal trends in risk-adjusted survival. After adjusting for patient and cardiac arrest characteristics, risk-adjusted rates of out-of-hospital cardiac arrest survival increased from 5.7% in the reference period of 2005 to 2006 to 7.2% in 2008 (adjusted risk ratio, 1.27; 95% confidence interval, 1.12-1.43; P<0.001). Survival improved more modestly to 8.3% in 2012 (adjusted risk ratio, 1.47; 95% confidence interval, 1.26-1.70; P<0.001). This improvement in survival occurred in both shockable and nonshockable arrest rhythms (P for interaction=0.22) and was also accompanied by better neurological outcomes among survivors (P for trend=0.01). Improved survival was attributable to both higher rates of prehospital survival, where risk-adjusted rates increased from 14.3% in 2005 to 2006 to 20.8% in 2012 (P for trend<0.001), and in-hospital survival (P for trend=0.015). Rates of bystander cardiopulmonary resuscitation and automated external defibrillator use modestly increased during the study period and partly accounted for prehospital survival trends.
Conclusions: Data drawn from a large subset of U.S communities suggest that rates of survival from out-of-hospital cardiac arrest have improved among sites participating in a performance improvement registry.
Keywords: cardiac arrest; survival; trends.
© 2014 American Heart Association, Inc.
Figures
Comment in
-
Treatment for out-of-hospital cardiac arrest: is the glass half empty or half full?Circulation. 2014 Nov 18;130(21):1844-6. doi: 10.1161/CIRCULATIONAHA.114.013263. Circulation. 2014. PMID: 25399398 No abstract available.
References
-
- Sasson C, Rogers MA, Dahl J, Kellermann AL. Predictors of survival from out-of-hospital cardiac arrest: a systematic review and meta-analysis. Circ Cardiovasc Qual Outcomes. 2010;3:63–81. - PubMed
-
- Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N Engl J Med. 2002;346:549–556. - PubMed
-
- Bernard SA, Gray TW, Buist MD, Jones BM, Silvester W, Gutteridge G, Smith K. Treatment of comatose survivors of out-of-hospital cardiac arrest with induced hypothermia. N Engl J Med. 2002;346:557–563. - PubMed
-
- Hallstrom AP, Ornato JP, Weisfeldt M, Travers A, Christenson J, McBurnie MA, Zalenski R, Becker LB, Schron EB, Proschan M. Public-access defibrillation and survival after out-of-hospital cardiac arrest. N Engl J Med. 2004;351:637–646. - PubMed
-
- Valenzuela TD, Roe DJ, Nichol G, Clark LL, Spaite DW, Hardman RG. Outcomes of rapid defibrillation by security officers after cardiac arrest in casinos. N Engl J Med. 2000;343:1206–1209. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
