

Twelve or 30 months of dual antiplatelet therapy after drug-eluting stents
- PMID: 25399658
- PMCID: PMC4481318
- DOI: 10.1056/NEJMoa1409312
Twelve or 30 months of dual antiplatelet therapy after drug-eluting stents
Abstract
Background: Dual antiplatelet therapy is recommended after coronary stenting to prevent thrombotic complications, yet the benefits and risks of treatment beyond 1 year are uncertain.
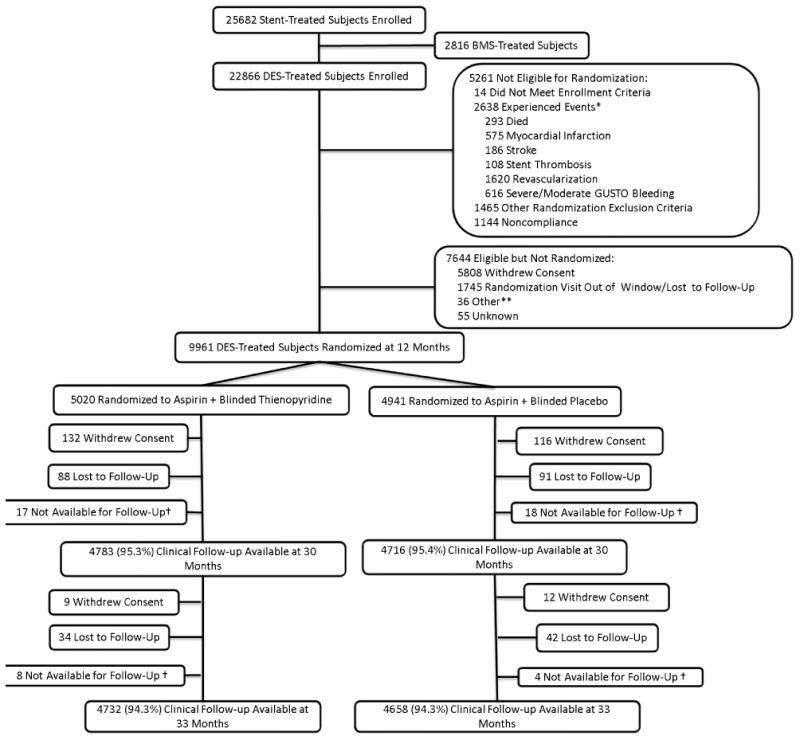
Methods: Patients were enrolled after they had undergone a coronary stent procedure in which a drug-eluting stent was placed. After 12 months of treatment with a thienopyridine drug (clopidogrel or prasugrel) and aspirin, patients were randomly assigned to continue receiving thienopyridine treatment or to receive placebo for another 18 months; all patients continued receiving aspirin. The coprimary efficacy end points were stent thrombosis and major adverse cardiovascular and cerebrovascular events (a composite of death, myocardial infarction, or stroke) during the period from 12 to 30 months. The primary safety end point was moderate or severe bleeding.
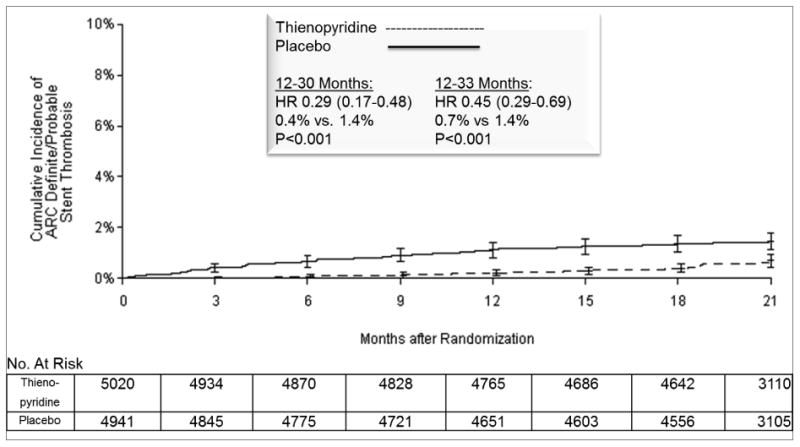
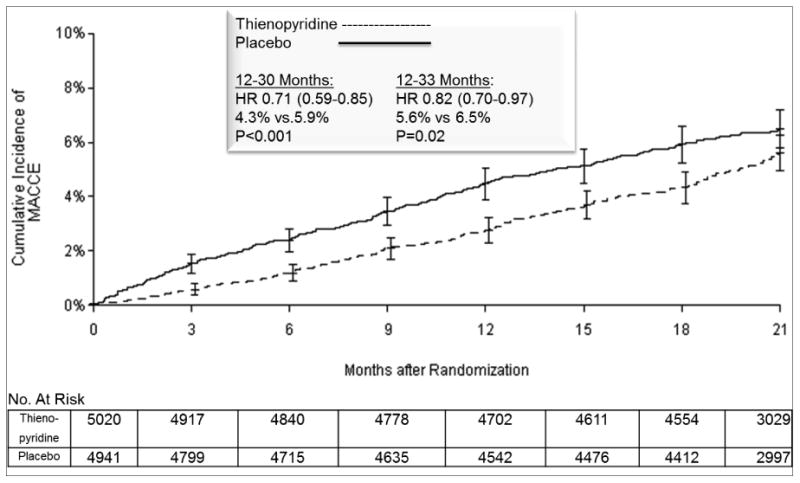
Results: A total of 9961 patients were randomly assigned to continue thienopyridine treatment or to receive placebo. Continued treatment with thienopyridine, as compared with placebo, reduced the rates of stent thrombosis (0.4% vs. 1.4%; hazard ratio, 0.29 [95% confidence interval {CI}, 0.17 to 0.48]; P<0.001) and major adverse cardiovascular and cerebrovascular events (4.3% vs. 5.9%; hazard ratio, 0.71 [95% CI, 0.59 to 0.85]; P<0.001). The rate of myocardial infarction was lower with thienopyridine treatment than with placebo (2.1% vs. 4.1%; hazard ratio, 0.47; P<0.001). The rate of death from any cause was 2.0% in the group that continued thienopyridine therapy and 1.5% in the placebo group (hazard ratio, 1.36 [95% CI, 1.00 to 1.85]; P=0.05). The rate of moderate or severe bleeding was increased with continued thienopyridine treatment (2.5% vs. 1.6%, P=0.001). An elevated risk of stent thrombosis and myocardial infarction was observed in both groups during the 3 months after discontinuation of thienopyridine treatment.
Conclusions: Dual antiplatelet therapy beyond 1 year after placement of a drug-eluting stent, as compared with aspirin therapy alone, significantly reduced the risks of stent thrombosis and major adverse cardiovascular and cerebrovascular events but was associated with an increased risk of bleeding. (Funded by a consortium of eight device and drug manufacturers and others; DAPT ClinicalTrials.gov number, NCT00977938.).
Figures
Comment in
-
Dual antiplatelet therapy after drug-eluting stents--how long to treat?N Engl J Med. 2014 Dec 4;371(23):2225-6. doi: 10.1056/NEJMe1413297. Epub 2014 Nov 16. N Engl J Med. 2014. PMID: 25399657 No abstract available.
-
Antiplatelet therapy: risks and benefits of extended DAPT after stenting.Nat Rev Cardiol. 2015 Jan;12(1):1. doi: 10.1038/nrcardio.2014.192. Epub 2014 Dec 2. Nat Rev Cardiol. 2015. PMID: 25445134 No abstract available.
-
Prolonged dual antiplatelet therapy after drug-eluting stent reduces the risk of stent thrombosis and major cardiovascular events but increases the rate of bleeding.Evid Based Med. 2015 Jun;20(3):99. doi: 10.1136/ebmed-2015-110167. Epub 2015 Mar 5. Evid Based Med. 2015. PMID: 25743171 No abstract available.
-
Balancing the risks and benefits of dual platelet inhibition.N Engl J Med. 2015 May 7;372(19):1854-6. doi: 10.1056/NEJMe1502137. Epub 2015 Mar 14. N Engl J Med. 2015. PMID: 25773507 No abstract available.
-
ACP journal club. Dual antiplatelets for 30 mo after drug-eluting stents reduced stent thrombosis and CV and cerebrovascular events.Ann Intern Med. 2015 Mar 17;162(6):JC9. doi: 10.7326/ACPJC-2015-162-6-009. Ann Intern Med. 2015. PMID: 25775352 No abstract available.
-
Duration of dual antiplatelet therapy after drug-eluting stents.N Engl J Med. 2015 Apr 2;372(14):1373-4. doi: 10.1056/NEJMc1501195. N Engl J Med. 2015. PMID: 25830429 No abstract available.
-
Duration of dual antiplatelet therapy after drug-eluting stents.N Engl J Med. 2015 Apr 2;372(14):1371. doi: 10.1056/NEJMc1501195. N Engl J Med. 2015. PMID: 25830430 No abstract available.
-
Duration of dual antiplatelet therapy after drug-eluting stents.N Engl J Med. 2015 Apr 2;372(14):1371. doi: 10.1056/NEJMc1501195. N Engl J Med. 2015. PMID: 25830431 No abstract available.
-
Duration of dual antiplatelet therapy after drug-eluting stents.N Engl J Med. 2015 Apr 2;372(14):1372. doi: 10.1056/NEJMc1501195. N Engl J Med. 2015. PMID: 25830432 No abstract available.
-
Duration of dual antiplatelet therapy after drug-eluting stents.N Engl J Med. 2015 Apr 2;372(14):1372. doi: 10.1056/NEJMc1501195. N Engl J Med. 2015. PMID: 25830433 No abstract available.
-
Duration of dual antiplatelet therapy after drug-eluting stents.N Engl J Med. 2015 Apr 2;372(14):1372-3. doi: 10.1056/NEJMc1501195. N Engl J Med. 2015. PMID: 25830434 No abstract available.
References
-
- Togni M, Balmer F, Pfiffner D, Maier W, Zeiher AM, Meier B. Percutaneous coronary interventions in Europe 1992-2001. Eur Heart J. 2004;25:1208–13. - PubMed
-
- Mauri L, Hsieh WH, Massaro JM, Ho KK, D'Agostino R, Cutlip DE. Stent thrombosis in randomized clinical trials of drug-eluting stents. N Engl J Med. 2007;356:1020–9. - PubMed
-
- Stone GW, Maehara A, Lansky AJ, et al. A prospective natural-history study of coronary atherosclerosis. N Engl J Med. 2011;364:226–35. - PubMed
-
- Cutlip DE, Chhabra AG, Baim DS, et al. Beyond restenosis: five-year clinical outcomes from second-generation coronary stent trials. Circulation. 2004;110:1226–30. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical