

Predictors of blood pressure response in the SYMPLICITY HTN-3 trial
- PMID: 25400162
- PMCID: PMC4301597
- DOI: 10.1093/eurheartj/ehu441
Predictors of blood pressure response in the SYMPLICITY HTN-3 trial
Abstract
Aims: The SYMPLICITY HTN-3 randomized, blinded, sham-controlled trial confirmed the safety of renal denervation (RDN), but did not meet its primary efficacy endpoint. Prior RDN studies have demonstrated significant and durable reductions in blood pressure. This analysis investigated factors that may help explain these disparate results.
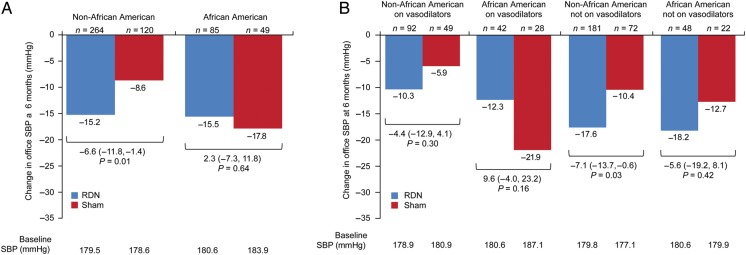
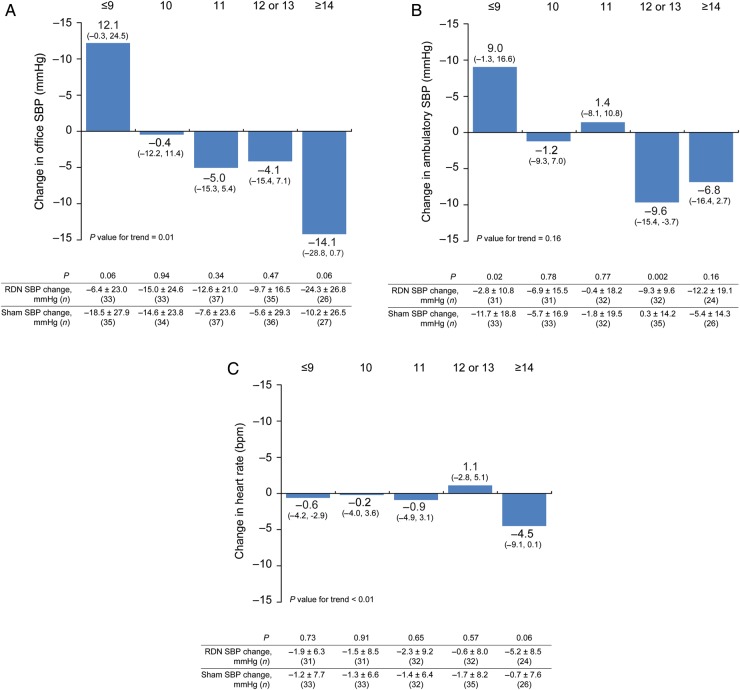
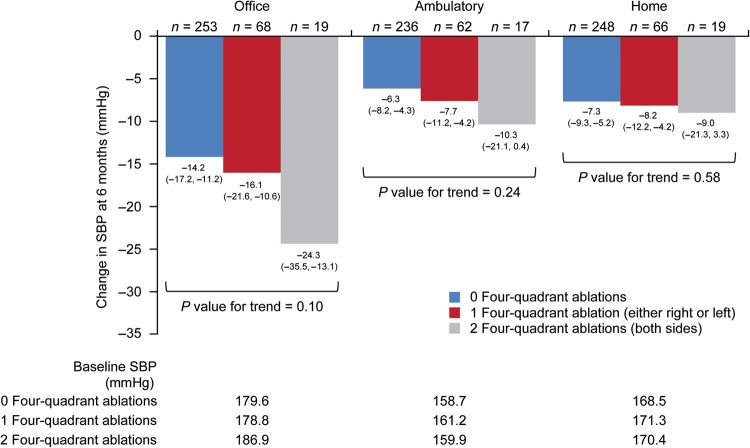
Methods and results: Patients with resistant hypertension were randomized 2 : 1 to RDN (n = 364) or sham (n = 171). The primary endpoint was the difference in office systolic blood pressure (SBP) change at 6 months. A multivariable analysis identified predictors of SBP change. Additional analyses examined the influence of medication changes, results in selected subgroups and procedural factors. Between randomization and the 6-month endpoint, 39% of patients underwent medication changes. Predictors of office SBP reduction at 6 months were baseline office SBP ≥ 180 mmHg, aldosterone antagonist use, and non-use of vasodilators; number of ablations was a predictor in the RDN group. Non-African-American patients receiving RDN had a significantly greater change in office SBP than those receiving sham; -15.2 ± 23.5 vs. -8.6 ± 24.8 mmHg, respectively (P = 0.012). Greater reductions in office and ambulatory SBP, and heart rate were observed with a higher number of ablations and energy delivery in a four-quadrant pattern.
Conclusions: Post hoc analyses, although derived from limited patient cohorts, reveal several potential confounding factors that may partially explain the unexpected blood pressure responses in both the sham control and RDN groups. These hypothesis-generating data further inform the design of subsequent research to evaluate the potential role of RDN in the treatment of resistant hypertension. CLINICALTRIALS.GOV IDENTIFIER: NCT01418261.
Keywords: Renal denervation; Resistant hypertension; SYMPLICITY.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author 2014. For permissions please email: journals.permissions@oup.com.
Figures
Comment in
-
Renal denervation: symply trapped by complexity?Eur Heart J. 2015 Jan 21;36(4):199-202. doi: 10.1093/eurheartj/ehu450. Epub 2014 Nov 16. Eur Heart J. 2015. PMID: 25400163 No abstract available.
Similar articles
-
SYMPLICITY HTN-Japan - First Randomized Controlled Trial of Catheter-Based Renal Denervation in Asian Patients -.Circ J. 2015;79(6):1222-9. doi: 10.1253/circj.CJ-15-0150. Epub 2015 Apr 24. Circ J. 2015. PMID: 25912693 Clinical Trial.
-
Long-term outcomes after catheter-based renal artery denervation for resistant hypertension: final follow-up of the randomised SYMPLICITY HTN-3 Trial.Lancet. 2022 Oct 22;400(10361):1405-1416. doi: 10.1016/S0140-6736(22)01787-1. Epub 2022 Sep 18. Lancet. 2022. PMID: 36130612 Clinical Trial.
-
12-month blood pressure results of catheter-based renal artery denervation for resistant hypertension: the SYMPLICITY HTN-3 trial.J Am Coll Cardiol. 2015 Apr 7;65(13):1314-1321. doi: 10.1016/j.jacc.2015.01.037. J Am Coll Cardiol. 2015. PMID: 25835443 Clinical Trial.
-
Effects of renal denervation on blood pressure in patients with hypertension: a latest systematic review and meta-analysis of randomized sham-controlled trials.Hypertens Res. 2024 Oct;47(10):2745-2759. doi: 10.1038/s41440-024-01739-y. Epub 2024 Jun 3. Hypertens Res. 2024. PMID: 38831091
-
Is the failure of SYMPLICITY HTN-3 trial to meet its efficacy endpoint the "end of the road" for renal denervation?J Am Soc Hypertens. 2015 Feb;9(2):140-9. doi: 10.1016/j.jash.2014.12.002. Epub 2014 Dec 11. J Am Soc Hypertens. 2015. PMID: 25649995 Review.
Cited by
-
Non-invasive Renal Denervation: Update on External Ultrasound Approaches.Curr Hypertens Rep. 2016 Jun;18(6):48. doi: 10.1007/s11906-016-0653-6. Curr Hypertens Rep. 2016. PMID: 27137523 Review.
-
Renal denervation for the treatment of hypertension: If at first you don't succeed, try and try again.Indian Heart J. 2015 May-Jun;67(3):192-3. doi: 10.1016/j.ihj.2015.03.021. Epub 2015 Apr 27. Indian Heart J. 2015. PMID: 26138171 Free PMC article. No abstract available.
-
Renal denervation for treatment of uncontrolled hypertension in an Asian population: results from the Global SYMPLICITY Registry in South Korea (GSR Korea).J Hum Hypertens. 2016 May;30(5):315-21. doi: 10.1038/jhh.2015.77. Epub 2015 Jul 9. J Hum Hypertens. 2016. PMID: 26155994
-
Global- and renal-specific sympathoinhibition in aldosterone hypertension.Hypertension. 2015 Jun;65(6):1223-30. doi: 10.1161/HYPERTENSIONAHA.115.05155. Epub 2015 Apr 20. Hypertension. 2015. PMID: 25895584 Free PMC article.
-
[Austrian Consensus on High Blood Pressure 2019].Wien Klin Wochenschr. 2019 Nov;131(Suppl 6):489-590. doi: 10.1007/s00508-019-01565-0. Wien Klin Wochenschr. 2019. PMID: 31792659 German.
References
-
- Smithwick RH, Thompson JE. Splanchnicectomy for essential hypertension; results in 1,266 cases. J Am Med Assoc. 1953;152:1501–1504. - PubMed
-
- Longland CJ, Gibb WE. Sympathectomy in the treatment of benign and malignant hypertension; a review of 76 patients. Br J Surg. 1954;41:382–392. - PubMed
-
- Esler M, Jennings G, Korner P, Willett I, Dudley F, Hasking G, Anderson W, Lambert G. Assessment of human sympathetic nervous system activity from measurements of norepinephrine turnover. Hypertension. 1988;11:3–20. - PubMed
-
- Esler M, Lambert G, Jennings G, Turner A, Kaye D. Central and peripheral norepinephrine kinetics in heart failure, coronary artery disease, and hypertension. Adv Pharmacol. 1998;42:650–653. - PubMed
-
- DiBona GF, Esler M. Translational medicine: the antihypertensive effect of renal denervation. Am J Physiol Regul Integr Comp Physiol. 2010;298:R245–R253. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
