

Cirrhotic cardiomyopathy: a cardiologist's perspective
- PMID: 25400434
- PMCID: PMC4229515
- DOI: 10.3748/wjg.v20.i42.15492
Cirrhotic cardiomyopathy: a cardiologist's perspective
Abstract
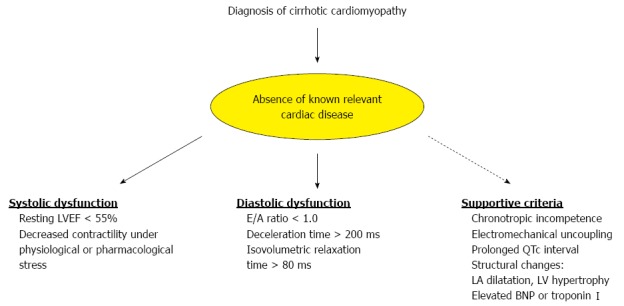
Cardiac dysfunction is frequently observed in patients with cirrhosis, and has long been linked to the direct toxic effect of alcohol. Cirrhotic cardiomyopathy (CCM) has recently been identified as an entity regardless of the cirrhosis etiology. Increased cardiac output due to hyperdynamic circulation is a pathophysiological hallmark of the disease. The underlying mechanisms involved in pathogenesis of CCM are complex and involve various neurohumoral and cellular pathways, including the impaired β-receptor and calcium signaling, altered cardiomyocyte membrane physiology, elevated sympathetic nervous tone and increased activity of vasodilatory pathways predominantly through the actions of nitric oxide, carbon monoxide and endocannabinoids. The main clinical features of CCM include attenuated systolic contractility in response to physiologic or pharmacologic strain, diastolic dysfunction, electrical conductance abnormalities and chronotropic incompetence. Particularly the diastolic dysfunction with impaired ventricular relaxation and ventricular filling is a prominent feature of CCM. The underlying mechanism of diastolic dysfunction in cirrhosis is likely due to the increased myocardial wall stiffness caused by myocardial hypertrophy, fibrosis and subendothelial edema, subsequently resulting in high filling pressures of the left ventricle and atrium. Currently, no specific treatment exists for CCM. The liver transplantation is the only established effective therapy for patients with end-stage liver disease and associated cardiac failure. Liver transplantation has been shown to reverse systolic and diastolic dysfunction and the prolonged QT interval after transplantation. Here, we review the pathophysiological basis and clinical features of cirrhotic cardiomyopathy, and discuss currently available limited therapeutic options.
Keywords: Cardiomyopathy; Cirrhosis; Diastolic dysfunction; Hyperdynamic circulation; Pathogenesis.
Figures
References
-
- Gerbes AL, Remien J, Jüngst D, Sauerbruch T, Paumgartner G. Evidence for down-regulation of beta-2-adrenoceptors in cirrhotic patients with severe ascites. Lancet. 1986;1:1409–1411. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
