

Extrahepatic complications to cirrhosis and portal hypertension: haemodynamic and homeostatic aspects
- PMID: 25400435
- PMCID: PMC4229516
- DOI: 10.3748/wjg.v20.i42.15499
Extrahepatic complications to cirrhosis and portal hypertension: haemodynamic and homeostatic aspects
Abstract
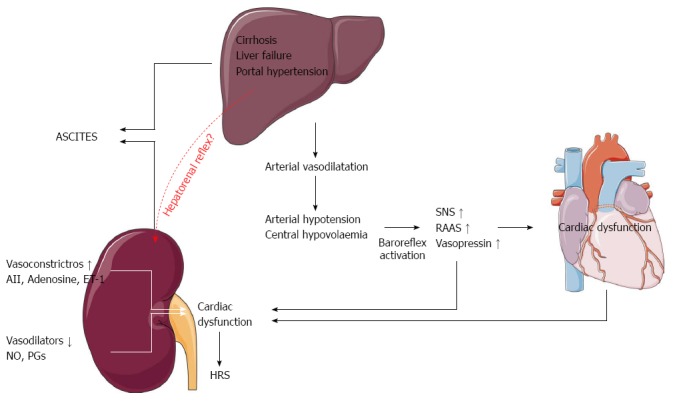
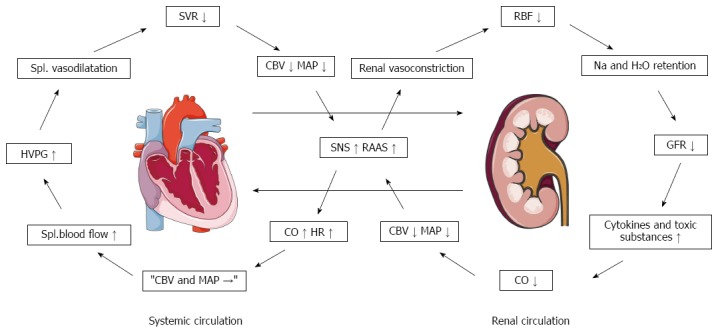
In addition to complications relating to the liver, patients with cirrhosis and portal hypertension develop extrahepatic functional disturbances of multiple organ systems. This can be considered a multiple organ failure that involves the heart, lungs, kidneys, the immune systems, and other organ systems. Progressive fibrosis of the liver and subsequent metabolic impairment leads to a systemic and splanchnic arteriolar vasodilatation. This affects both the haemodynamic and functional homeostasis of many organs and largely determines the course of the disease. With the progression of the disease, the circulation becomes hyperdynamic with cardiac, pulmonary as well as renal consequences for dysfunction and reduced survival. Infections and a changed cardiac function known as cirrhotic cardiomyopathy may be involved in further aggravation of other complications such as renal failure precipitating the hepatorenal syndrome. Patients with end-stage liver disease and related complications as for example the hepatopulmonary syndrome can only radically be treated by liver transplantation. As a bridge to this treatment, knowledge on the mechanisms of the pathophysiology of complications is essential for the choice of vasoactive drugs, antibiotics, drugs with specific effects on fibrogenesis and inflammation, and drugs that target specific receptors.
Keywords: Ascites; Bacterial translocation; Cirrhotic cardiomyopathy; Fibrogenesis; Hepatopulmonary syndrome; Hepatorenal syndrome; Infections; Inflammation; Portopulmonary hypertension; Splanchnic haemodynamics; Systemic circulation.
Figures


References
-
- 11th ed. Oxford: Wiley-Blackwell; 2002. Sherlock’s Diseases of the Liver and Biliary system.
-
- García-Pagán JC, Gracia-Sancho J, Bosch J. Functional aspects on the pathophysiology of portal hypertension in cirrhosis. J Hepatol. 2012;57:458–461. - PubMed
-
- Bendtsen F, Krag A, Møller S. Treatment of acute variceal bleeding. Dig Liver Dis. 2008;40:328–336. - PubMed
-
- Bosch J, Abraldes JG, Fernández M, García-Pagán JC. Hepatic endothelial dysfunction and abnormal angiogenesis: new targets in the treatment of portal hypertension. J Hepatol. 2010;53:558–567. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
