

Covert hepatic encephalopathy: agreement and predictive validity of different indices
- PMID: 25400460
- PMCID: PMC4229541
- DOI: 10.3748/wjg.v20.i42.15756
Covert hepatic encephalopathy: agreement and predictive validity of different indices
Abstract
Aim: To investigate the agreement and prognostic value of different measures of covert hepatic encephalopathy (CHE).
Methods: One-hundred-and-thirty-two cirrhotic outpatients underwent electroencephalography (EEG), paper-and-pencil psychometry (PHES) and critical flicker frequency, scored on the original/modified (CFFo/CFFm) thresholds. Eighty-four patients underwent Doppler-ultrasound to diagnose/exclude portal-systemic shunt. Seventy-nine were followed-up for 11 ± 7 mo in relation to the occurrence of hepatic encephalopathy (HE)-related hospitalisations.
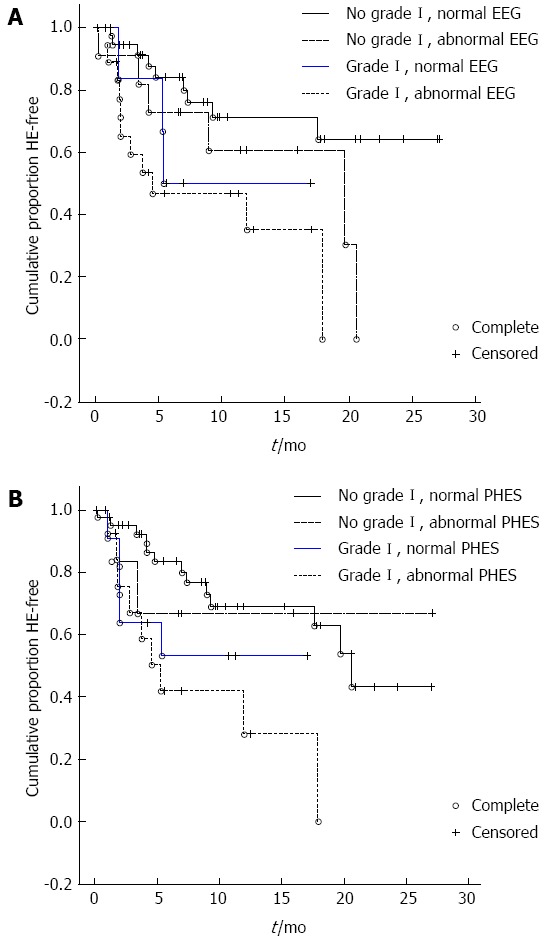
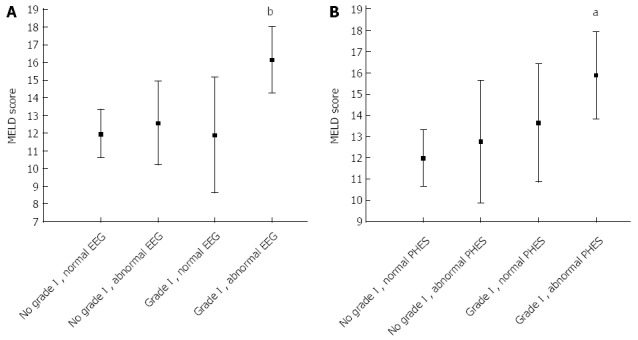
Results: On the day of study, 36% had grade I HE, 42% abnormal EEG, 33% abnormal PHES and 31/21% abnormal CFFo/CFFm. Significant associations were observed between combinations of test abnormalities; however, agreement was poor (Cohen's κ < 0.4). The prevalence of EEG, PHES and CFFo/CFFm abnormalities was significantly higher in patients with grade I overt HE. The prevalence of EEG and CFFm abnormalities was higher in patients with shunt. The prevalence of EEG abnormalities was significantly higher in patients with a history of HE. During follow-up, 10 patients died, 10 were transplanted and 29 had HE-related hospitalisations. Grade I HE (P = 0.004), abnormal EEG (P = 0.008) and abnormal PHES (P = 0.04) at baseline all predicted the subsequent occurrence of HE; CFF did not.
Conclusion: CHE diagnosis probably requires a combination of clinical, neurophysiological and neuropsychological indices.
Keywords: Ammonia; Electroencephalography; Hepatic encephalopathy; Liver cirrhosis; Psychometry.
Figures
References
-
- Kircheis G, Fleig WE, Görtelmeyer R, Grafe S, Häussinger D. Assessment of low-grade hepatic encephalopathy: a critical analysis. J Hepatol. 2007;47:642–650. - PubMed
-
- Ferenci P, Lockwood A, Mullen K, Tarter R, Weissenborn K, Blei AT. Hepatic encephalopathy--definition, nomenclature, diagnosis, and quantification: final report of the working party at the 11th World Congresses of Gastroenterology, Vienna, 1998. Hepatology. 2002;35:716–721. - PubMed
-
- Bajaj JS, Cordoba J, Mullen KD, Amodio P, Shawcross DL, Butterworth RF, Morgan MY. Review article: the design of clinical trials in hepatic encephalopathy--an International Society for Hepatic Encephalopathy and Nitrogen Metabolism (ISHEN) consensus statement. Aliment Pharmacol Ther. 2011;33:739–747. - PMC - PubMed
-
- Pugh RN, Murray-Lyon IM, Dawson JL, Pietroni MC, Williams R. Transection of the oesophagus for bleeding oesophageal varices. Br J Surg. 1973;60:646–649. - PubMed
-
- Kamath PS, Wiesner RH, Malinchoc M, Kremers W, Therneau TM, Kosberg CL, D’Amico G, Dickson ER, Kim WR. A model to predict survival in patients with end-stage liver disease. Hepatology. 2001;33:464–470. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
