

Overview of the cellular and molecular basis of kidney fibrosis
- PMID: 25401038
- PMCID: PMC4220516
- DOI: 10.1038/kisup.2014.2
Overview of the cellular and molecular basis of kidney fibrosis
Abstract
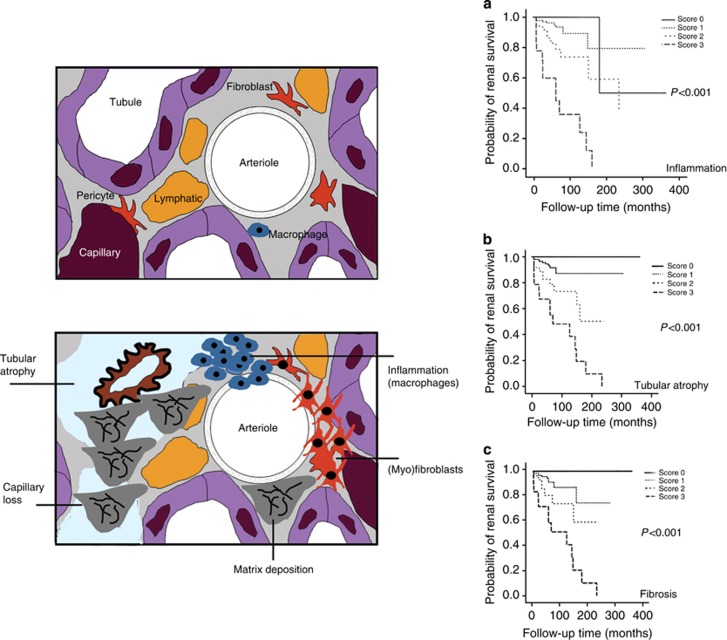
The common pathogenetic pathway of progressive injury in patients with chronic kidney disease (CKD) is epitomized as normal kidney parenchymal destruction due to scarring (fibrosis). Understanding the fundamental pathways that lead to renal fibrosis is essential in order to develop better therapeutic options for human CKD. Although complex, four cellular responses are pivotal. (1) An interstitial inflammatory response that has multiple consequences-some harmful and others healing. (2) The appearance of a unique interstitial cell population of myofibroblasts, primarily derived from kidney stromal cells (fibroblasts and pericytes), that are the primary source of the various extracellular matrix proteins that form interstitial scars. (3) Tubular epithelial cells that have variable and time-dependent roles as early responders to injury and later as victims of fibrosis due to the loss of their regenerative abilities. (4) Loss of interstitial capillary integrity that compromises oxygen delivery and leads to a vicious cascade of hypoxia-oxidant stress that accentuates injury and fibrosis. In the absence of adequate angiogenic responses, a healthy interstitial capillary network is not maintained. The fibrotic 'scar' that typifies CKD is an interesting consortium of multifunctional macromolecules that not only change in composition and structure over time, but can be degraded via extracellular and intracellular proteases. Although transforming growth factor beta appears to be the primary driver of kidney fibrosis, a vast array of additional molecules may have modulating roles. The importance of genetic and epigenetic factors is increasingly appreciated. An intriguing but incompletely understood cardiorenal syndrome underlies the high morbidity and mortality rates that develop in association with progressive kidney fibrosis.
Keywords: extracellular matrix; interstitial capillaries; kidney fibrosis; macrophages; myofibroblasts.
Figures
References
-
- Yu F, Wu LH, Tan Y, et al. Tubulointerstitial lesions of patients with lupus nephritis classified by the 2003 International Society of Nephrology and Renal Pathology Society system. Kidney Int. 2010;77:820–829. - PubMed
-
- Eddy AA, Neilson EG. Chronic kidney disease progression. J Am Soc Nephrol. 2006;17:2964–2966. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
