

Decrease in urinary creatinine excretion in early stage chronic kidney disease
- PMID: 25401694
- PMCID: PMC4234219
- DOI: 10.1371/journal.pone.0111949
Decrease in urinary creatinine excretion in early stage chronic kidney disease
Abstract
Background: Little is known about muscle mass loss in early stage chronic kidney disease (CKD). We used 24-hour urinary creatinine excretion rate to assess determinants of muscle mass and its evolution with kidney function decline. We also described the range of urinary creatinine concentration in this population.
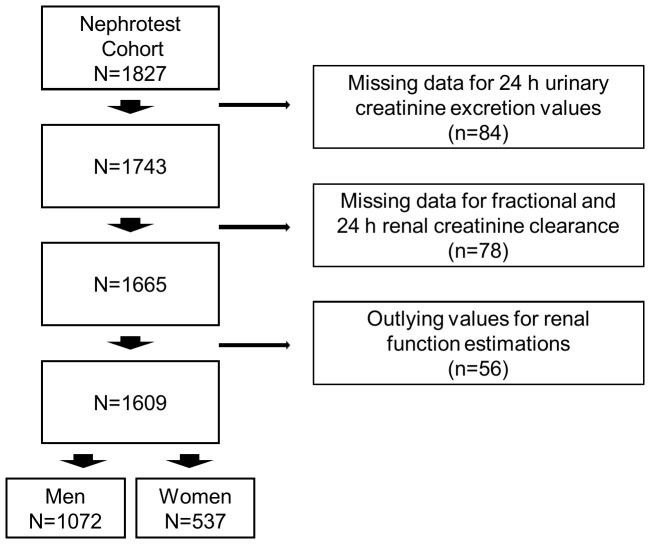
Methods: We included 1072 men and 537 women with non-dialysis CKD stages 1 to 5, all of them with repeated measurements of glomerular filtration rate (mGFR) by (51)Cr-EDTA renal clearance and several nutritional markers. In those with stage 1 to 4 at baseline, we used a mixed model to study factors associated with urinary creatinine excretion rate and its change over time.
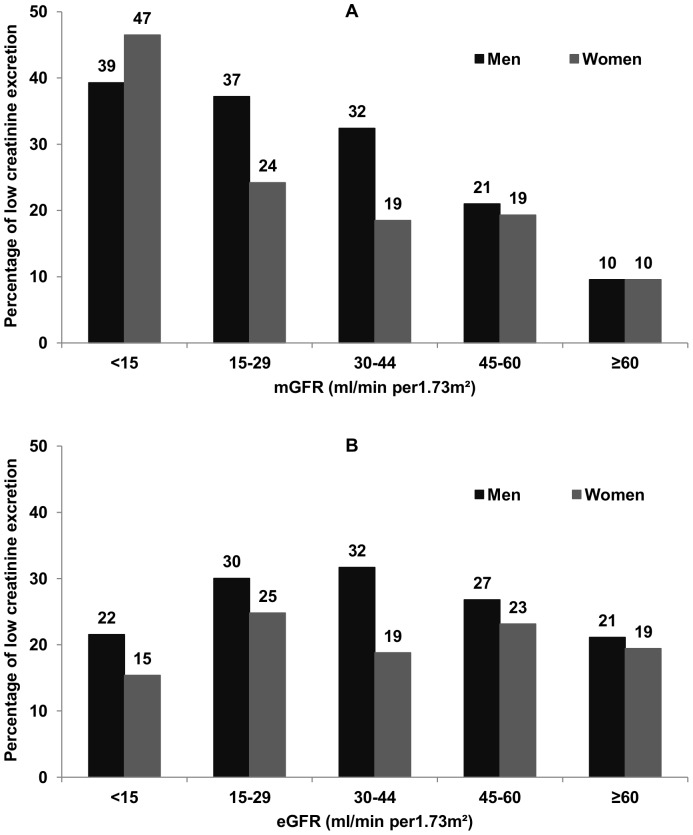
Results: Baseline mean urinary creatinine excretion decreased from 15.3 ± 3.1 to 12.1 ± 3.3 mmol/24 h (0.20 ± 0.03 to 0.15 ± 0.04 mmol/kg/24 h) in men, with mGFR falling from ≥ 60 to <15 mL/min/1.73 m(2), and from 9.6 ± 1.9 to 7.6 ± 2.5 (0.16 ± 0.03 to 0.12 ± 0.03) in women. In addition to mGFR, an older age, diabetes, and lower levels of body mass index, proteinuria, and protein intake assessed by urinary urea were associated with lower mean urinary creatinine excretion at baseline. Mean annual decline in mGFR was 1.53 ± 0.12 mL/min/1.73 m(2) per year and that of urinary creatinine excretion rate, 0.28 ± 0.02 mmol/24 h per year. Patients with fast annual decline in mGFR of 5 mL/min/1.73 m(2) had a decrease in urinary creatinine excretion more than twice as big as in those with stable mGFR, independent of changes in urinary urea as well as of other determinants of low muscle mass.
Conclusions: Decrease in 24-hour urinary creatinine excretion rate may appear early in CKD patients, and is greater the more mGFR declines independent of lowering protein intake assessed by 24-hour urinary urea. Normalizing urine analytes for creatininuria may overestimate their concentration in patients with reduced kidney function and low muscle mass.
Conflict of interest statement
Figures
References
-
- Kalantar-Zadeh K, Ikizler TA, Block G, Avram MM, Kopple JD (2003) Malnutrition-inflammation complex syndrome in dialysis patients: causes and consequences. Am J Kidney Dis Off J Natl Kidney Found 42: 864–881. - PubMed
-
- Blumenkrantz MJ, Kopple JD, Gutman RA, Chan YK, Barbour GL, et al. (1980) Methods for assessing nutritional status of patients with renal failure. Am J Clin Nutr 33: 1567–1585. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
