

Evaluation of the National Comprehensive Cancer Network and American Urological Association renal cell carcinoma surveillance guidelines
- PMID: 25403213
- PMCID: PMC4265116
- DOI: 10.1200/JCO.2014.56.5416
Evaluation of the National Comprehensive Cancer Network and American Urological Association renal cell carcinoma surveillance guidelines
Abstract
Purpose: The National Comprehensive Cancer Network (NCCN) and American Urological Association (AUA) provide guidelines for surveillance after surgery for renal cell carcinoma (RCC). Herein, we assess the ability of the guidelines to capture RCC recurrences and determine the duration of surveillance required to capture 90%, 95%, and 100% of recurrences.
Patients and methods: We evaluated 3,651 patients who underwent surgery for M0 RCC between 1970 and 2008. Patients were stratified as AUA low risk (pT1Nx-0) after partial (LR-partial) or radical nephrectomy (LR-radical) or as moderate/high risk (M/HR; pT2-4Nx-0/pTanyN1). Guidelines were assessed by calculating the percentage of recurrences detected when following the 2013 and 2014 NCCN and AUA recommendations, and associated Medicare costs were compared.
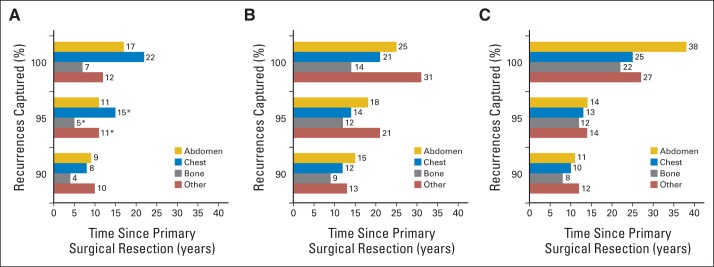
Results: At a median follow-up of 9.0 years (interquartile range, 5.7 to 14.4 years), a total of 1,088 patients (29.8%) experienced a recurrence. Of these, 390 recurrences (35.9%) were detected using 2013 NCCN recommendations, 742 recurrences (68.2%) were detected using 2014 NCCN recommendations, and 728 recurrences (66.9%) were detected using AUA recommendations. All protocols missed the greatest amount of recurrences in the abdomen and among pT1Nx-0 patients. To capture 95% of recurrences, surveillance was required for 15 years for LR-partial, 21 years for LR-radical, and 14 years for M/HR patients. Medicare surveillance costs for one LR-partial patient were $1,228.79 using 2013 NCCN, $2,131.52 using 2014 NCCN, and $1,738.31 using AUA guidelines. However, if 95% of LR-partial recurrences were captured, costs would total $9,856.82.
Conclusion: If strictly followed, the 2014 NCCN and AUA guidelines will miss approximately one third of RCC recurrences. Improved surveillance algorithms, which balance patient benefits and health care costs, are needed.
© 2014 by American Society of Clinical Oncology.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
Comment in
-
Is extending surveillance guidelines for renal cell carcinoma without understanding patient outcomes putting the cart before the horse?J Clin Oncol. 2014 Dec 20;32(36):4031-2. doi: 10.1200/JCO.2014.58.3195. Epub 2014 Nov 17. J Clin Oncol. 2014. PMID: 25403216 No abstract available.
-
Re: Evaluation of the National Comprehensive Cancer Network and American Urological Association Renal Cell Carcinoma Surveillance Guidelines.J Urol. 2015 Jul;194(1):43. doi: 10.1016/j.juro.2015.04.048. Epub 2015 Apr 16. J Urol. 2015. PMID: 26088219 No abstract available.
References
-
- Skolarikos A, Alivizatos G, Laguna P, et al. A review on follow-up strategies for renal cell carcinoma after nephrectomy. Eur Urol. 2007;51:1490–1500. - PubMed
-
- Montie JE. Follow-up after partial or total nephrectomy for renal cell carcinoma. Urol Clin North Am. 1994;21:589–592. - PubMed
-
- Sandock DS, Seftel AD, Resnick MI. A new protocol for the followup of renal cell carcinoma based on pathological stage. J Urol. 1995;154:28–31. - PubMed
-
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Kidney Cancer 2.2014. http://www.nccn.org/professionals/physician_gls/pdf/kidney.pdf. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
