

The changing clinical profile of celiac disease: a 15-year experience (1998-2012) in an Italian referral center
- PMID: 25404189
- PMCID: PMC4236812
- DOI: 10.1186/s12876-014-0194-x
The changing clinical profile of celiac disease: a 15-year experience (1998-2012) in an Italian referral center
Abstract
Background: Celiac disease is a multiform, challenging condition characterized by extremely variable features. Our goal was to define clinical, serological and histopathological findings in a large cohort of celiacs diagnosed in a single referral center.
Methods: From January 1998 to December 2012, 770 patients (599 females, median age 36 years, range 18-78 years) were diagnosed as celiacs at St. Orsola-Malpighi Hospital (Bologna, Italy). The clinical phenotypes were classified as: 1) classical (malabsorption syndrome); 2) non-classical (extraintestinal and/or gastrointestinal symptoms other than diarrhea); 3) subclinical. Serology, duodenal histology, comorbidities, response to gluten-free diet and complications were evaluated.
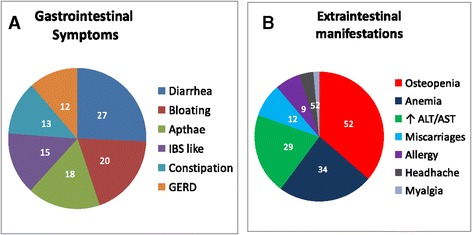
Results: Disease onset was symptomatic in 610 patients (79%), while 160 celiacs showed a subclinical phenotype. In the symptomatic group the non-classical prevailed over the classical phenotype (66% vs 34%). Diarrhea was found in 27%, while other gastrointestinal manifestations were bloating (20%), aphthous stomatitis (18%), alternating bowel habit (15%), constipation (13%) and gastroesophageal reflux disease (12%). Extraintestinal manifestations included osteopenia/osteoporosis (52%), anemia (34%), cryptogenic hypertransaminasemia (29%) and recurrent miscarriages (12%). Positivity for IgA tissue transglutaminase antibodies was detected in 97%. Villous atrophy was found in 87%, while 13% had minor lesions consistent with potential celiac disease. A large proportion of patients showed autoimmune disorders, i.e. autoimmune thyroiditis (26.3%), dermatitis herpetiformis (4%) and diabetes mellitus type 1 (3%). Complicated celiac disease was very rare.
Conclusions: Our study demonstrates that the clinical profile of celiac disease changed over time with an increasing rate of non-classical and subclinical phenotypes.
Figures


References
-
- Karell K, Louka AS, Moodie SJ, Ascher H, Clot F, Greco L, Ciclitira PJ, Sollid LM, Partanen J, European Genetics Cluster on Celiac Disease HLA types in celiac disease patients not carrying the DQA1*05-DQB1*02 (DQ2) heterodimer: results from the European Genetics Cluster on Celiac Disease. Hum Immunol. 2003;64:469–477. doi: 10.1016/S0198-8859(03)00027-2. - DOI - PubMed
-
- Ivarsson A, Hernell O, Stenlund H, Persson LA. Breast-feeding protects against celiac disease. Am J Clin Nutr. 2002;75:914–921. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
