

Common harms from amoxicillin: a systematic review and meta-analysis of randomized placebo-controlled trials for any indication
- PMID: 25404399
- PMCID: PMC4284189
- DOI: 10.1503/cmaj.140848
Common harms from amoxicillin: a systematic review and meta-analysis of randomized placebo-controlled trials for any indication
Abstract
Background: When prescribing antibiotics for common indications, clinicians need information about both harms and benefits, information that is currently available only from observational studies. We quantified the common harms of the most frequently prescribed antibiotic, amoxicillin, from randomized placebo-controlled trials.
Methods: For this systematic review, we searched MEDLINE, Embase and the Cochrane Central Register of Controlled Trials, without language restriction, for any randomized, participant-blinded, placebo-controlled trials of amoxicillin or amoxicillin-clavulanic acid for any indication, in any setting. Our main outcome was any reported adverse event.
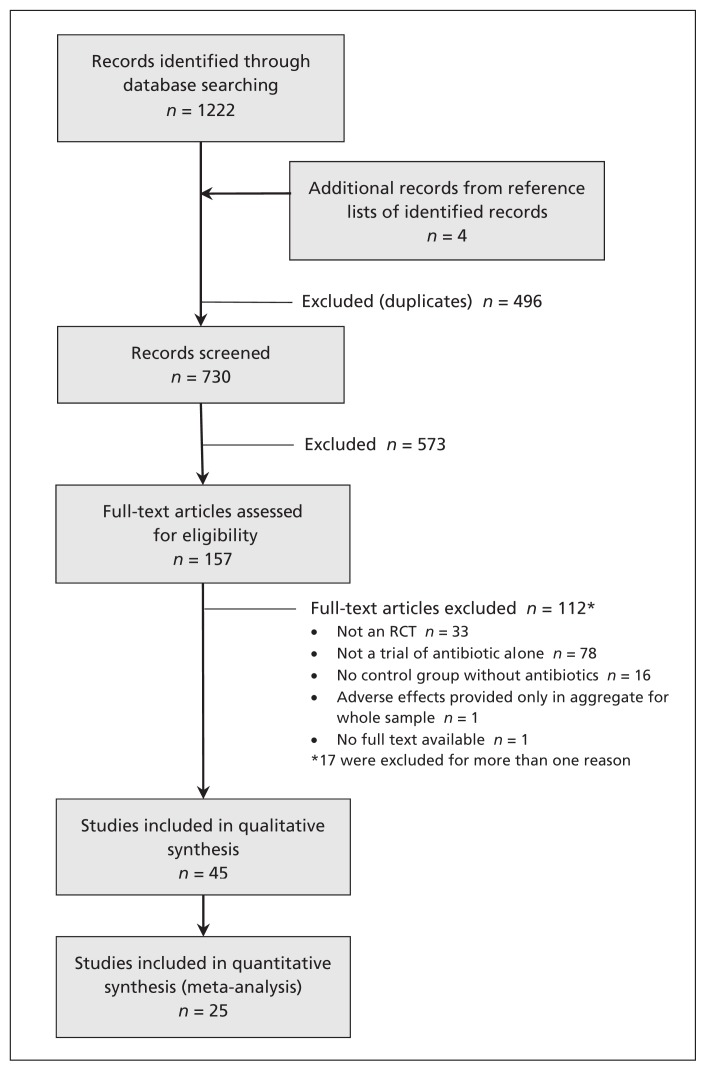
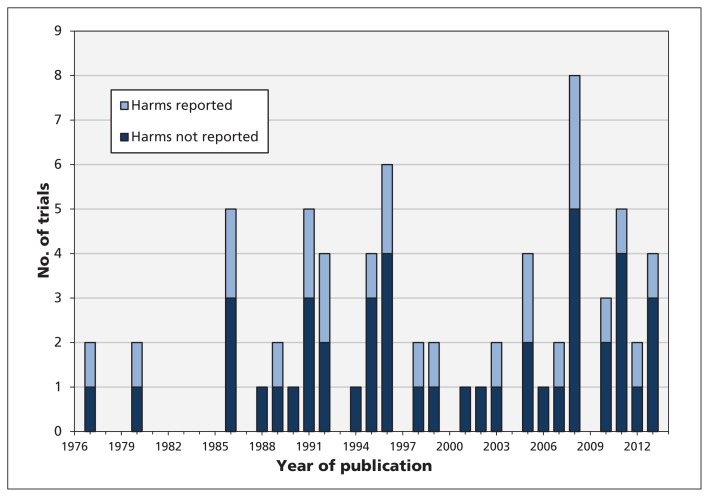
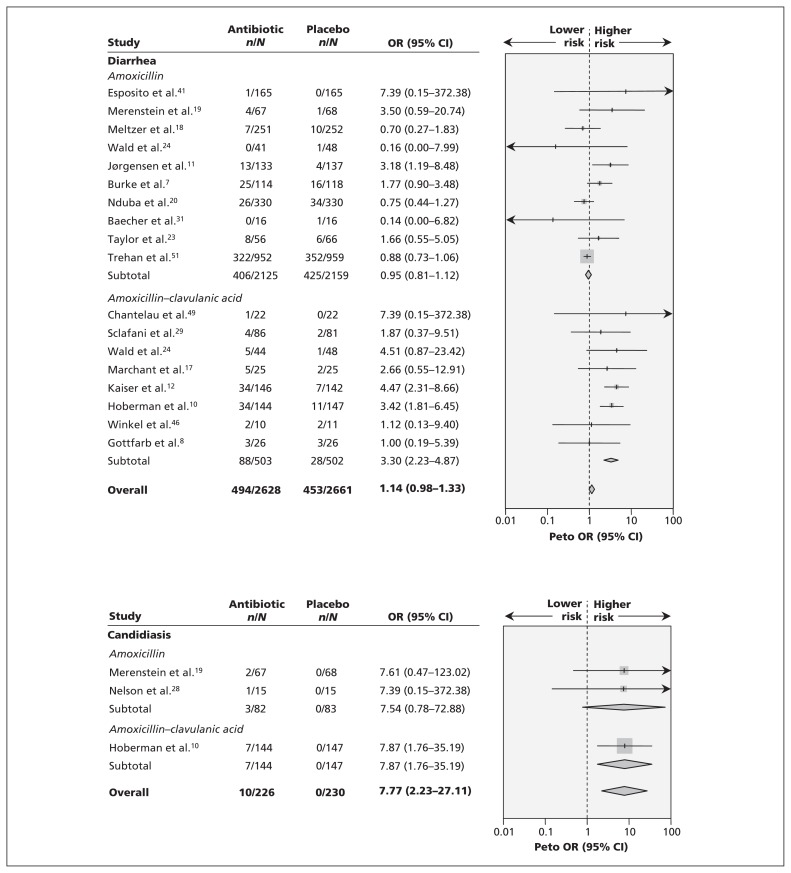
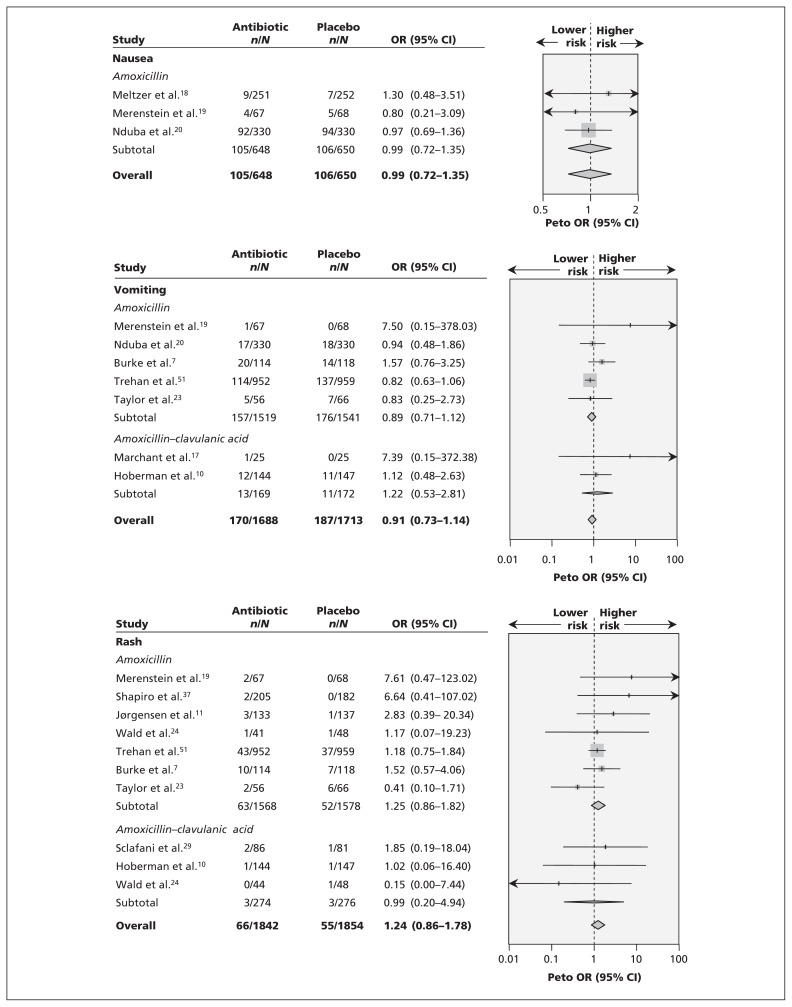
Results: Of 730 studies identified, we included 45 trials: 27 involving amoxicillin, 17 involving amoxicillin-clavulanic acid and 1 involving both. The indications for antibiotic therapy were variable. The risk of bias was low, although only 25 trials provided data suitable for assessment of harms, which suggested under-reporting. Diarrhea was attributed to amoxicillin only in the form of amoxicillin-clavulanic acid (Peto odds ratio [OR] 3.30, 95% confidence interval [CI] 2.23-4.87). The OR for candidiasis (3 trials) was significantly higher (OR 7.77, 95% CI 2.23-27.11). Rashes, nausea, itching, vomiting and abnormal results on liver function tests were not significantly increased. The results were not altered by sensitivity analyses, nor did funnel plots suggest publication bias. The number of courses of antibiotics needed to harm was 10 (95% CI 6-17) for diarrhea with amoxicillin-clavulanic acid and 27 (95% CI 24-42) for candidiasis with amoxicillin (with or without clavulanic acid).
Interpretation: Diarrhea was caused by use of amoxicillin-clavulanic acid, and candidiasis was caused by both amoxicillin and amoxicillin-clavulanic acid. Harms were poorly reported in most trials, and their true incidence may have been higher than reported. Nevertheless, these rates of common harms associated with amoxicillin therapy may inform decisions by helping clinicians to balance harms against benefits.
© 2015 Canadian Medical Association or its licensors.
Figures
Comment in
-
If nothing happens, is everything all right? Distinguishing genuine reassurance from a false sense of security.CMAJ. 2015 Jan 6;187(1):15-16. doi: 10.1503/cmaj.141344. Epub 2014 Nov 17. CMAJ. 2015. PMID: 25404394 Free PMC article. No abstract available.
-
Penicillin VK oral suspension.CMAJ. 2015 Apr 7;187(6):439. doi: 10.1503/cmaj.115-0025. CMAJ. 2015. PMID: 25852177 Free PMC article. No abstract available.
-
Group A streptococcus.CMAJ. 2015 Apr 21;187(7):521. doi: 10.1503/cmaj.115-0032. CMAJ. 2015. PMID: 25897171 Free PMC article. No abstract available.
References
-
- Tan T, Little P, Stokes TGuideline Development Group. Antibiotic prescribing for self limiting respiratory tract infections in primary care: summary of NICE guidance. BMJ 2008;337:a437. - PubMed
-
- Cosby JL, Francis N, Butler CC. The role of evidence in the decline of antibiotic use for common respiratory infections in primary care. Lancet Infect Dis 2007;7:749–56. - PubMed
-
- Higgins JPT, Green S, editors. Cochrane handbook for systematic reviews of interventions. Version 5.1.0. Oxford (UK): Cochrane Collaboration; 2011. Available: www.handbook.cochrane.org (accessed 2014 Sept. 25).
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical