

Costs of health resource utilization among HIV-positive individuals in British Columbia, Canada: results from a population-level study
- PMID: 25404425
- PMCID: PMC4677778
- DOI: 10.1007/s40273-014-0229-8
Costs of health resource utilization among HIV-positive individuals in British Columbia, Canada: results from a population-level study
Abstract
Background: Through delayed HIV disease progression, highly active antiretroviral therapy (HAART) may reduce direct medical costs, thus at least partially offsetting therapy costs. Recent findings regarding the secondary preventive benefits of HAART necessitate careful consideration of funding allocations for HIV/AIDS care. Our objective is to estimate non-HAART direct medical costs at different levels of disease progression and over time in British Columbia, Canada.
Methods: We considered the population of individuals with HIV/AIDS within a set of linked disease registries and health administrative databases (N = 11,836) from 1996 to 2010. Costs of hospitalization, physician billing, diagnostic testing and non-HAART medications were calculated in 2010 Canadian dollars. Effects of covariates on quarterly costs were assessed with a two-part model with logit for probability of non-zero costs and a generalized linear model (GLM). Net effects of CD4 strata on direct non-HAART medical costs were evaluated over time during the study period.
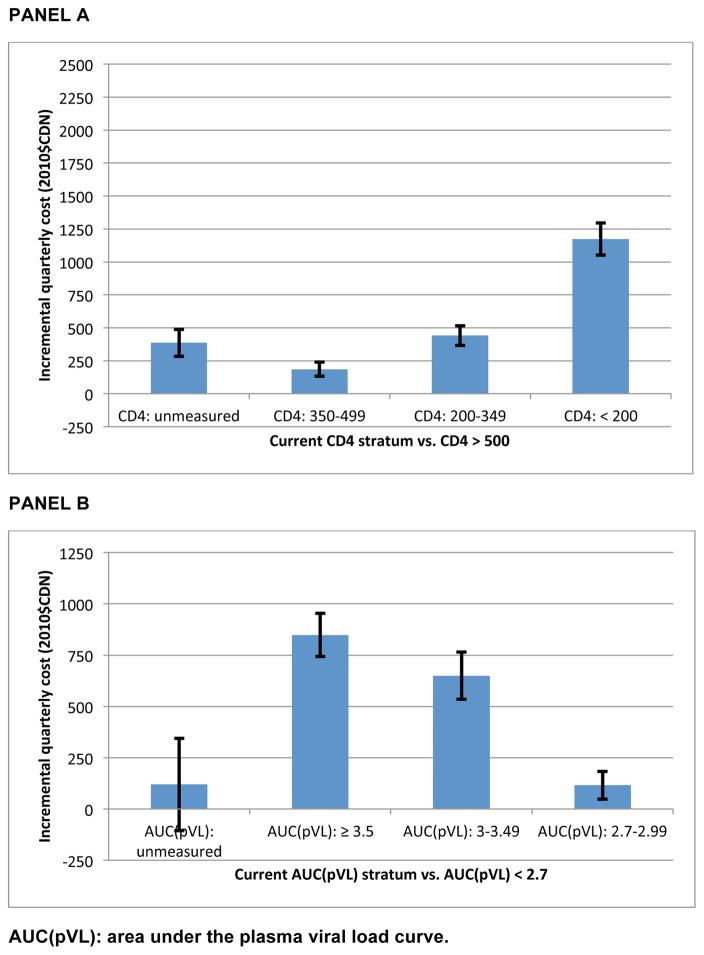
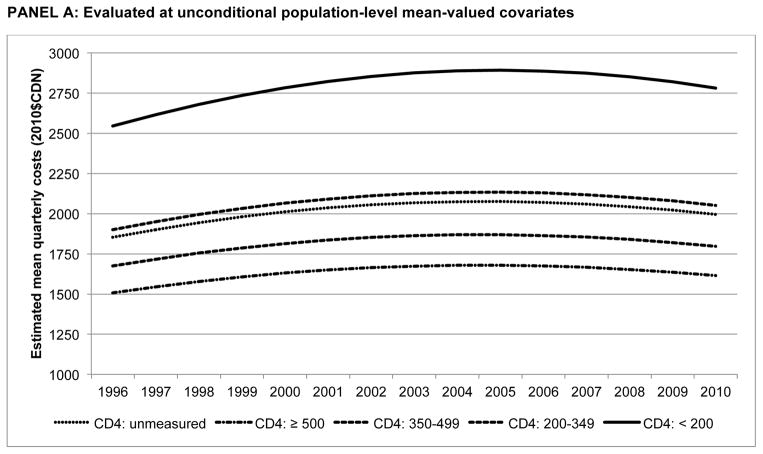
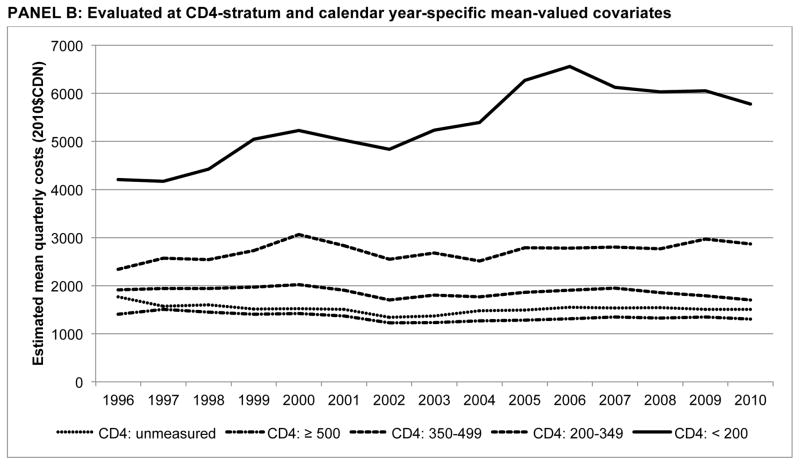
Results: Compared with person-quarters in which CD4 >500/mm(3), costs were Can$185 (95 % confidence interval [CI] 132-239) greater for CD4 350-500/mm(3), Can$441 (95 % CI 366-516) greater for CD4 200-350/mm(3) and Can$1,173 (95 % CI 1,051-1,294) greater when CD4 <200/mm(3). Prior to HIV care initiation, individuals incurred costs Can$385 (95 % CI 283-487) greater than in periods with CD4 >500/mm(3). Hospitalization comprised the majority of the increment in costs amongst those with no measured CD4. Evaluated at CD4 state conditional means, those with CD4 <200/mm(3) incurred quarterly costs of Can$5,781 (95 % CI 4,716-6,846) versus Can$1,307 (95 % CI 1,154-1,460; p < 0.001) for CD4 ≥500/mm(3) in 2010.
Conclusion: Non-HAART direct medical costs were substantially lower for individuals during periods of sustained virologic suppression and high CD4 count. HIV treatment and prevention evaluations require detailed health resource use data to inform funding allocation decisions.
Conflict of interest statement
Figures
References
-
- Hogg RS, O’Shaughnessy MV, Gataric N, et al. Decline in deaths from AIDS due to new antiretrovirals. Lancet. 1997;349:1294. - PubMed
-
- Walensky RP, Paltiel AD, Losina E, et al. The survival benefi ts of AIDS treatment in the United States. J Infect Dis. 2006;194:11–19. - PubMed
-
- Bozzette SA, Joce G, McCaffrey DF, et al. Expenditures for the care of HIV-infected patients in the era of highly active antiretroviral therapy. N Engl J Med. 2001;344:817–23. - PubMed
-
- Chen RY, Accort NA, Westfall AO, et al. Distribution of health care expenditures for HIV-infected patients. Clinc Infect Dis. 2006;42:1003–10. - PubMed
-
- Sloan CE, Champenois K, Choisy P, Losina E, Walensky RP, Schackman BR, Ajana F, Melliez H, Paltiel AD, Freedberg KA, Yazdanpanah Y Cost-Effectiveness of Preventing AIDS Complications (CEPAC) investigators. Newer drugs and earlier treatment: impact on lifetime cost of care for HIV-infected adults. AIDS. 2012 Jan 2;26(1):45–56. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
