

Flap reconstruction of the knee: A review of current concepts and a proposed algorithm
- PMID: 25405089
- PMCID: PMC4133468
- DOI: 10.5312/wjo.v5.i5.603
Flap reconstruction of the knee: A review of current concepts and a proposed algorithm
Abstract
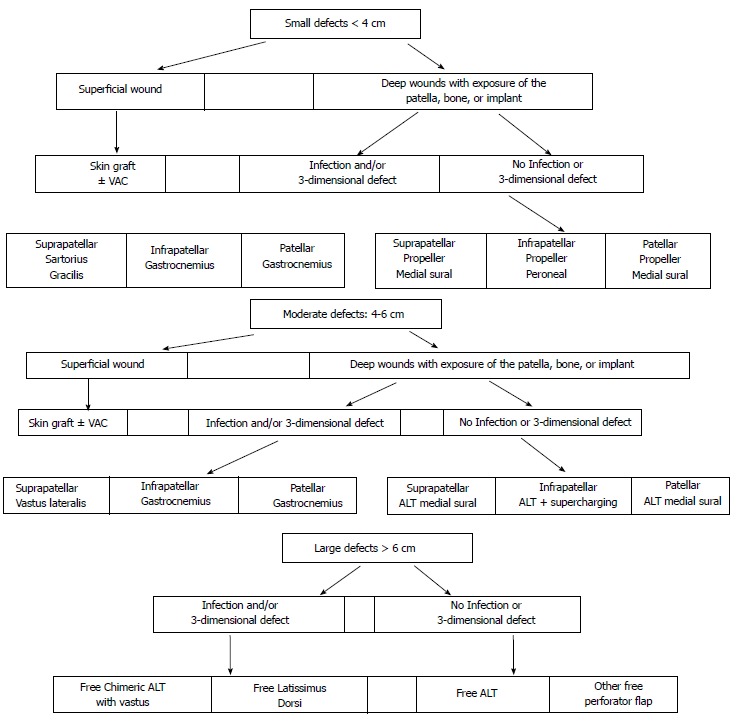
A literature search focusing on flap knee reconstruction revealed much controversy regarding the optimal management of around the knee defects. Muscle flaps are the preferred option, mainly in infected wounds. Perforator flaps have recently been introduced in knee coverage with significant advantages due to low donor morbidity and long pedicles with wide arc of rotation. In the case of free flap the choice of recipient vessels is the key point to the reconstruction. Taking the published experience into account, a reconstructive algorithm is proposed according to the size and location of the wound, the presence of infection and/or 3-dimensional defect.
Keywords: Free flap; Knee reconstruction; Local flap; Pedicled flap; Recipient vessels.
Figures

References
-
- Asko-Seljavaara S, Kilpi ML, Hytönen M, Sundell B. The burned hand. Early treatment and surgery of scars and contractions. Ann Chir Gynaecol. 1980;69:224–231. - PubMed
-
- Andres LA, Casey WJ, Clarke HD. Techniques in Soft Tissue Coverage Around the Knee. Techniques Knee Surg. 2009;8:119–125.
-
- Fang T, Zhang EW, Lineaweaver WC, Zhang F. Recipient vessels in the free flap reconstruction around the knee. Ann Plast Surg. 2013;71:429–433. - PubMed
-
- Panni AS, Vasso M, Cerciello S, Salgarello M. Wound complications in total knee arthroplasty. Which flap is to be used? With or without retention of prosthesis? Knee Surg Sports Traumatol Arthrosc. 2011;19:1060–1068. - PubMed
-
- Hill DS, O’Neill JK, Toms A, Watts AM. Pyoderma gangrenosum: a report of a rare complication after knee arthroplasty requiring muscle flap cover supplemented by negative pressure therapy and hyperbaric oxygen. J Plast Reconstr Aesthet Surg. 2011;64:1528–1532. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
