

Management of proximal humerus fractures in adults
- PMID: 25405098
- PMCID: PMC4133477
- DOI: 10.5312/wjo.v5.i5.685
Management of proximal humerus fractures in adults
Abstract
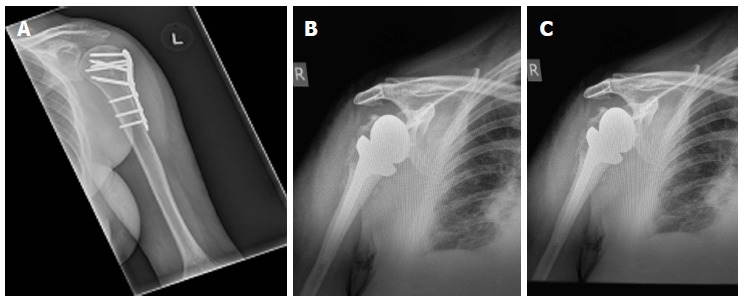
The majority of proximal humerus fractures are low-energy osteoporotic injuries in the elderly and their incidence is increasing in the light of an ageing population. The diversity of fracture patterns encountered renders objective classification of prognostic value challenging. Non-operative management has been associated with good functional outcomes in stable, minimally displaced and certain types of displaced fractures. Absolute indications for surgery are infrequent and comprise compound, pathological, multi-fragmentary head-splitting fractures and fracture dislocations, as well as those associated with neurovascular injury. A constantly expanding range of reconstructive and replacement options however has been extending the indications for surgical management of complex proximal humerus fractures. As a result, management decisions are becoming increasingly complicated, in an attempt to provide the best possible treatment for each individual patient, that will successfully address their specific fracture configuration, comorbidities and functional expectations. Our aim was to review the management options available for the full range of proximal humerus fractures in adults, along with their specific advantages, disadvantages and outcomes.
Keywords: Hemiarthroplasty; Non-operative management; Proximal humerus fracture; Reconstruction; Reverse polarity total shoulder arthroplasty.
Figures
References
-
- Horak J, Nilsson BE. Epidemiology of fracture of the upper end of the humerus. Clin Orthop Relat Res. 1975;(112):250–253. - PubMed
-
- Court-Brown CM, Caesar B. Epidemiology of adult fractures: A review. Injury. 2006;37:691–697. - PubMed
-
- Lind T, Krøner K, Jensen J. The epidemiology of fractures of the proximal humerus. Arch Orthop Trauma Surg. 1989;108:285–287. - PubMed
-
- Court-Brown CM, Garg A, McQueen MM. The epidemiology of proximal humeral fractures. Acta Orthop Scand. 2001;72:365–371. - PubMed
-
- Roux A, Decroocq L, El Batti S, Bonnevialle N, Moineau G, Trojani C, Boileau P, de Peretti F. Epidemiology of proximal humerus fractures managed in a trauma center. Orthop Traumatol Surg Res. 2012;98:715–719. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
