

A cluster randomised controlled trial of a pharmacist-led collaborative intervention to improve statin prescribing and attainment of cholesterol targets in primary care
- PMID: 25405478
- PMCID: PMC4236200
- DOI: 10.1371/journal.pone.0113370
A cluster randomised controlled trial of a pharmacist-led collaborative intervention to improve statin prescribing and attainment of cholesterol targets in primary care
Abstract
Background: Small trials with short term follow up suggest pharmacists' interventions targeted at healthcare professionals can improve prescribing. In comparison with clinical guidance, contemporary statin prescribing is sub-optimal and achievement of cholesterol targets falls short of accepted standards, for patients with atherosclerotic vascular disease who are at highest absolute risk and who stand to obtain greatest benefit. We hypothesised that a pharmacist-led complex intervention delivered to doctors and nurses in primary care, would improve statin prescribing and achievement of cholesterol targets for incident and prevalent patients with vascular disease, beyond one year.
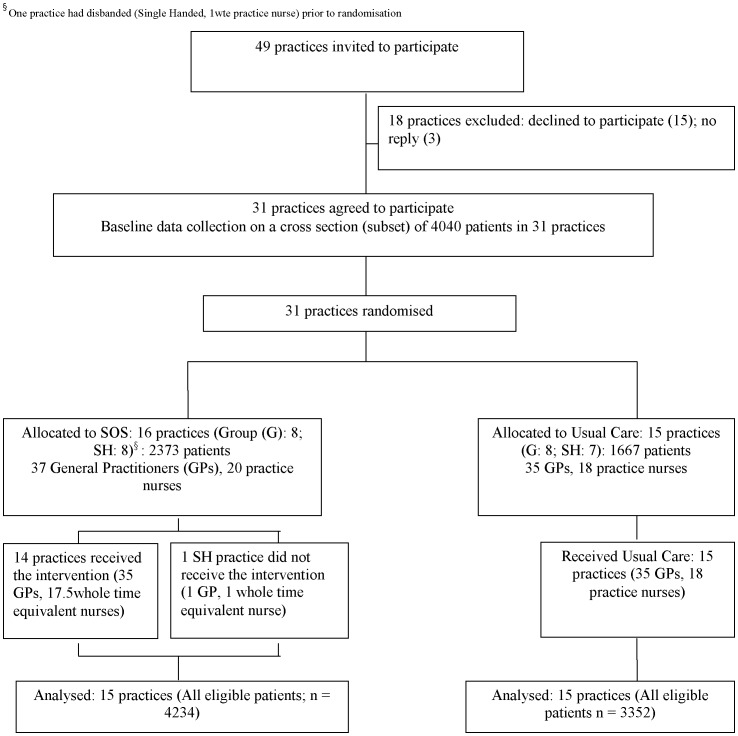
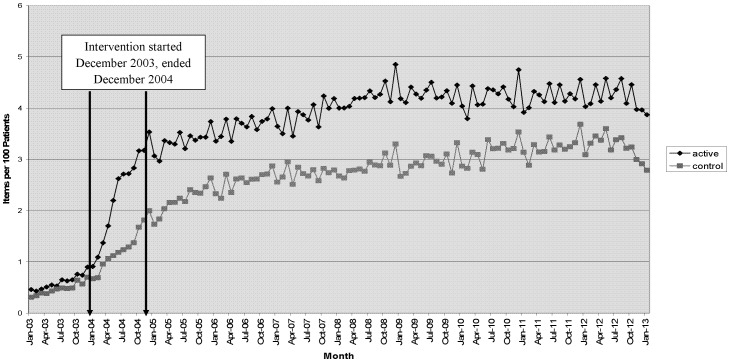
Methods: We allocated general practices to a 12-month Statin Outreach Support (SOS) intervention or usual care. SOS was delivered by one of 11 pharmacists who had received additional training. SOS comprised academic detailing and practical support to identify patients with vascular disease who were not prescribed a statin at optimal dose or did not have cholesterol at target, followed by individualised recommendations for changes to management. The primary outcome was the proportion of patients achieving cholesterol targets. Secondary outcomes were: the proportion of patients prescribed simvastatin 40 mg with target cholesterol achieved; cholesterol levels; prescribing of simvastatin 40 mg; prescribing of any statin and the proportion of patients with cholesterol tested. Outcomes were assessed after an average of 1.7 years (range 1.4-2.2 years), and practice level simvastatin 40 mg prescribing was assessed after 10 years.
Findings: We randomised 31 practices (72 General Practitioners (GPs), 40 nurses). Prior to randomisation a subset of eligible patients were identified to characterise practices; 40% had cholesterol levels below the target threshold. Improvements in data collection procedures allowed identification of all eligible patients (n = 7586) at follow up. Patients in practices allocated to SOS were significantly more likely to have cholesterol at target (69.5% vs 63.5%; OR 1.11, CI 1.00-1.23; p = 0.043) as a result of improved simvastatin prescribing. Subgroup analysis showed the primary outcome was achieved by prevalent but not incident patients. Statistically significant improvements occurred in all secondary outcomes for prevalent patients and all but one secondary outcome (the proportion of patients with cholesterol tested) for incident patients. SOS practices prescribed more simvastatin 40 mg than usual care practices, up to 10 years later.
Interpretation: Through a combination of educational and organisational support, a general practice based pharmacist led collaborative intervention can improve statin prescribing and achievement of cholesterol targets in a high-risk primary care based population.
Trial registration: International Standard Randomised Controlled Trials Register ISRCTN61233866.
Conflict of interest statement
Figures
Similar articles
-
A cluster randomised controlled trial of pharmacist led statin outreach support (SOS) in primary care: design and baseline characteristics.Contemp Clin Trials. 2010 Jul;31(4):303-11. doi: 10.1016/j.cct.2010.03.010. Epub 2010 Mar 27. Contemp Clin Trials. 2010. PMID: 20348032 Clinical Trial.
-
Effect of fixed dose combination treatment on adherence and risk factor control among patients at high risk of cardiovascular disease: randomised controlled trial in primary care.BMJ. 2014 May 27;348:g3318. doi: 10.1136/bmj.g3318. BMJ. 2014. PMID: 24868083 Clinical Trial.
-
Encouraging Pharmacist Referrals for Evidence-Based Statin Initiation: Two Cluster Randomized Clinical Trials.JAMA Cardiol. 2025 May 1;10(5):473-481. doi: 10.1001/jamacardio.2025.0244. JAMA Cardiol. 2025. PMID: 40136263 Clinical Trial.
-
Effects of pharmacist prescribing on patient outcomes in the hospital setting: a systematic review.JBI Database System Rev Implement Rep. 2018 Sep;16(9):1823-1873. doi: 10.11124/JBISRIR-2017-003697. JBI Database System Rev Implement Rep. 2018. PMID: 30204671
-
[Lipid therapy in daily routine].Dtsch Med Wochenschr. 2012 Oct;137(40):2047-52. doi: 10.1055/s-0032-1327203. Epub 2012 Sep 28. Dtsch Med Wochenschr. 2012. PMID: 23023622 Review. German.
Cited by
-
Reducing cardiovascular risk among people living with HIV: Rationale and design of the INcreasing Statin Prescribing in HIV Behavioral Economics REsearch (INSPIRE) randomized controlled trial.Prog Cardiovasc Dis. 2020 Mar-Apr;63(2):109-117. doi: 10.1016/j.pcad.2020.02.012. Epub 2020 Feb 19. Prog Cardiovasc Dis. 2020. PMID: 32084445 Free PMC article.
-
Pharmacists' perceptions of their emerging general practice roles in UK primary care: a qualitative interview study.Br J Gen Pract. 2017 Sep;67(662):e650-e658. doi: 10.3399/bjgp17X691733. Epub 2017 Jul 3. Br J Gen Pract. 2017. PMID: 28673959 Free PMC article.
-
The Excellence of Pharmacy Practice.Innov Pharm. 2020 Jan 28;11(1):10.24926/iip.v11i1.1662. doi: 10.24926/iip.v11i1.1662. eCollection 2020. Innov Pharm. 2020. Retraction in: Innov Pharm. 2020 Jan 28;11(1). doi: 10.24926/iip.v11i2.3944. PMID: 34017646 Free PMC article. Retracted. Review.
-
Clinical Pharmacist Outreach to Increase Statin Use for Patients with Cardiovascular Disease in a Safety-Net Healthcare System.Am Health Drug Benefits. 2021 Jun;14(2):63-69. Am Health Drug Benefits. 2021. PMID: 34267861 Free PMC article.
-
Vanderbilt Health Affiliated Network Statin Outreach Service.Clin Diabetes. 2020 Jul;38(3):295-299. doi: 10.2337/cd19-0099. Clin Diabetes. 2020. PMID: 32699480 Free PMC article.
References
-
- Lowrie R, Mair F, Greenlaw N, Forsyth P, Jhund P, et al. (2012) Pharmacist intervention in primary care to improve outcomes in patients with left ventricular systolic dysfunction. European Heart Journal 33(3): 314–324. - PubMed
-
- Thomson O’Brien MA, Oxman AD, Davis DA (2002) Educational Outreach visits: effects on professional practice and health care outcomes. The Cochrane Database of Systematic Reviews. The Cochrane Library. 1: 1. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
