

Computerized cognitive training in cognitively healthy older adults: a systematic review and meta-analysis of effect modifiers
- PMID: 25405755
- PMCID: PMC4236015
- DOI: 10.1371/journal.pmed.1001756
Computerized cognitive training in cognitively healthy older adults: a systematic review and meta-analysis of effect modifiers
Abstract
Background: New effective interventions to attenuate age-related cognitive decline are a global priority. Computerized cognitive training (CCT) is believed to be safe and can be inexpensive, but neither its efficacy in enhancing cognitive performance in healthy older adults nor the impact of design factors on such efficacy has been systematically analyzed. Our aim therefore was to quantitatively assess whether CCT programs can enhance cognition in healthy older adults, discriminate responsive from nonresponsive cognitive domains, and identify the most salient design factors.
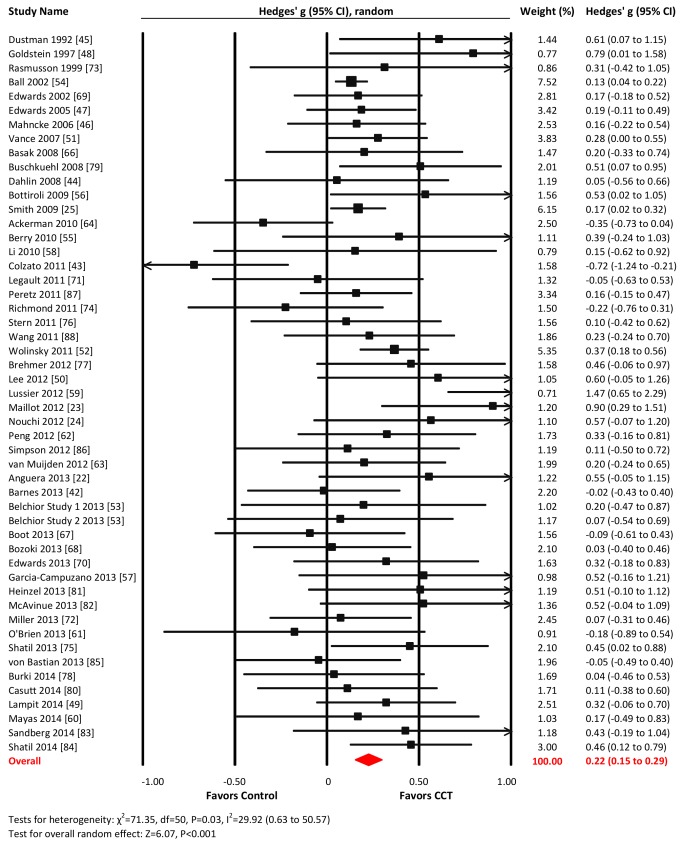
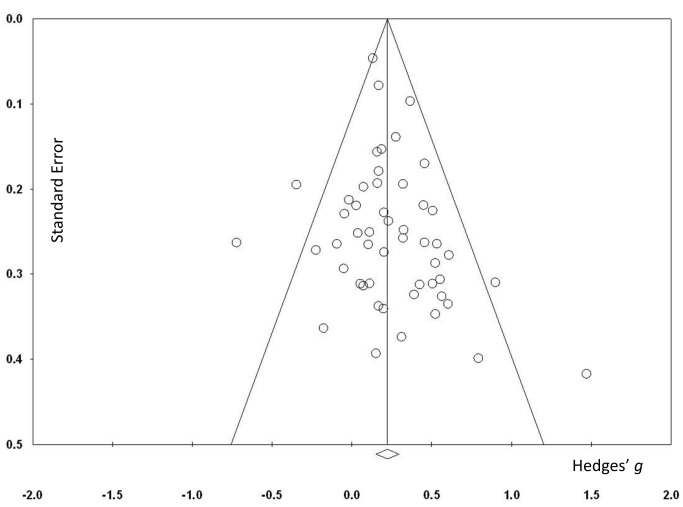
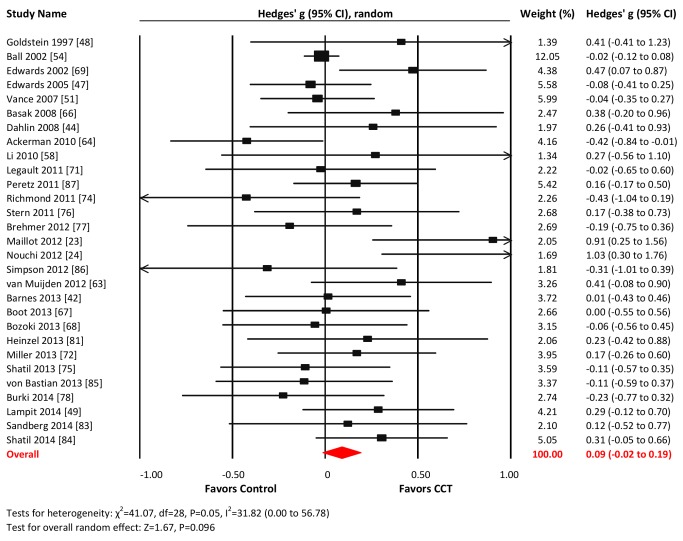
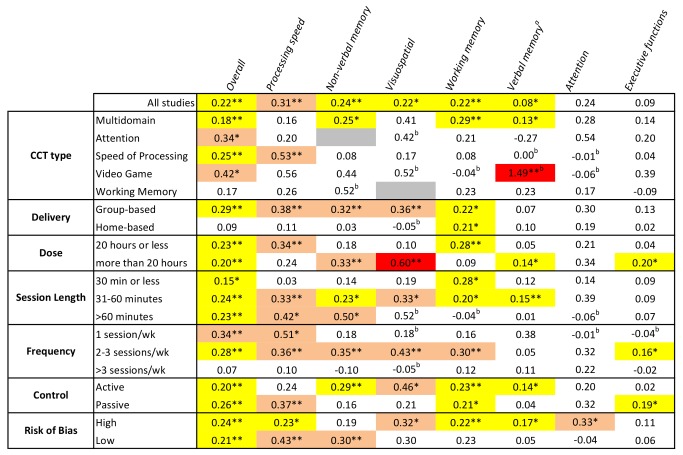
Methods and findings: We systematically searched Medline, Embase, and PsycINFO for relevant studies from the databases' inception to 9 July 2014. Eligible studies were randomized controlled trials investigating the effects of ≥ 4 h of CCT on performance in neuropsychological tests in older adults without dementia or other cognitive impairment. Fifty-two studies encompassing 4,885 participants were eligible. Intervention designs varied considerably, but after removal of one outlier, heterogeneity across studies was small (I(2) = 29.92%). There was no systematic evidence of publication bias. The overall effect size (Hedges' g, random effects model) for CCT versus control was small and statistically significant, g = 0.22 (95% CI 0.15 to 0.29). Small to moderate effect sizes were found for nonverbal memory, g = 0.24 (95% CI 0.09 to 0.38); verbal memory, g = 0.08 (95% CI 0.01 to 0.15); working memory (WM), g = 0.22 (95% CI 0.09 to 0.35); processing speed, g = 0.31 (95% CI 0.11 to 0.50); and visuospatial skills, g = 0.30 (95% CI 0.07 to 0.54). No significant effects were found for executive functions and attention. Moderator analyses revealed that home-based administration was ineffective compared to group-based training, and that more than three training sessions per week was ineffective versus three or fewer. There was no evidence for the effectiveness of WM training, and only weak evidence for sessions less than 30 min. These results are limited to healthy older adults, and do not address the durability of training effects.
Conclusions: CCT is modestly effective at improving cognitive performance in healthy older adults, but efficacy varies across cognitive domains and is largely determined by design choices. Unsupervised at-home training and training more than three times per week are specifically ineffective. Further research is required to enhance efficacy of the intervention. Please see later in the article for the Editors' Summary.
Conflict of interest statement
MV has received research funding and honoraria from the Brain Department LLC for a project unrelated to this work. His group also receives in-kind research support in the form of no-cost software from BrainTrain Inc (USA), also unrelated to this work.
Figures








Comment in
-
What could computerized brain training learn from evidence-based medicine?PLoS Med. 2014 Nov 18;11(11):e1001758. doi: 10.1371/journal.pmed.1001758. eCollection 2014 Nov. PLoS Med. 2014. PMID: 25405859 Free PMC article.
-
Computerised cognitive training programs improved the cognitive performance of healthy older adults on some cognitive tests including memory, speed of information processing and visuospatial skills.Aust Occup Ther J. 2015 Jun;62(3):223-4. doi: 10.1111/1440-1630.12209. Aust Occup Ther J. 2015. PMID: 26058781 No abstract available.
References
-
- Deary IJ, Corley J, Gow AJ, Harris SE, Houlihan LM, et al. (2009) Age-associated cognitive decline. Br Med Bull 92: 135–152. - PubMed
-
- Graham JE, Rockwood K, Beattie BL, Eastwood R, Gauthier S, et al. (1997) Prevalence and severity of cognitive impairment with and without dementia in an elderly population. Lancet 349: 1793–1796. - PubMed
-
- Unverzagt FW, Gao S, Baiyewu O, Ogunniyi AO, Gureje O, et al. (2001) Prevalence of cognitive impairment: data from the Indianapolis Study of Health and Aging. Neurology 57: 1655–1662. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
